Volume 13 • Issue 3 • 1J Surgery, an open access journalISSN: 1584-9341
Keywords: Sepsis; Biomarkers; Presepsin; Sepsis related mortality
IntroducereSepticemia este definită ca o boală infecţioasă, de cauză bacteriană,
ce evoluează ca o infecţie sistemică gravă ce va evolua către sepsis sever (o disfuncție acută de organ cauzată de o infecție sau suspicionată a fi cauzată de către o infecție) și către șoc septic(sepsis sever asociat cu hipotensiune ce nu răspunde la terapia de resuscitare volemică), instalată ca urmare a unor descărcări repetate în sânge de germeni patogeni, toxine și produşi de dezintegrare celulară. Sepsisul și formele sale clinice trebuie considerate ca fiind stadii ale aceleiași afecțiuni [1].
Cu toate progresele înregistrate în terapia antibiotică, sepsisul reprezintă în continuare un sindrom comun și cu implicații devastatoare asupra sistemelor de îngrijiri de sănatate la nivel mondial. Costul estimat mediu anual pentru îngrijirea pacienților cu sepsis a fost calculat la o valoare de 16,7 miliarde$, la nivelul anului 2008 [2].
Această patologie reprezintă o provocare pentru serviciile supraaglomerate de urgenţă. Nerecunoaşterea acestei entităţi la momentul oportun, urmată de iniţierea precoce a terapiei etiologice şi suportive poate duce la degradarea parametrilor vitali sau chiar la decesul acestor pacienţi. De aici decurge şi necesitatea folosirii unor metode de diagnostic paraclinic facil de utilizat, cu specificitate şi sensibilitate mare care să permită un diagnostic precoce, disponibil în timp scurt în departamentele de urgență.
Biomarkeri pot avea un rol important în a evidenția prezența și severitatea sepsisului [3-8]. Presepsina (sCD14-ST)-CD14, este o glicoproteină exprimată pe suprafața membranei celulare a monocitelor și a macrofagelor, prezentă și în macrofage, monocite și granulocite, fiind responsabilă de transmiterea intracelulară a semnalului declanșat de prezența endotoxinelor. Fracția sa solubilă, numită subtipul CD14 solubil sau presepsină, are nivele plasmatice crescute în infecții [6-8].
Valoarea cut-off a presepsinei, ce permite diferențierea sindromului
*Corresponding author: Diana Cimpoiesu, Emergency Department, “St Spiridon” Hospital, “Gr. T. Popa” University of Medicine and Pharmacy, Bd. Independentei No 1, Iasi, Romania, Tel: + 40 (0) 722 38 76 70; E-mail: [email protected]
Received June 24, 2015; Accepted May 05, 2017; Published June 12, 2017
Citation: Popa O, Cimpoiesu D, Dorobat C. Presepsin:Early Biomarker in Diagnosis of Sepsis in Emergency Department. Journal of Surgery [Jurnalul de chirurgie]. 2017; 13(3): 85-90 DOI: 10.7438/1584-9341-13-3-1 [article in Romanian]
AbstractObjective: Sepsis is a common syndrome with devastating implications for health care systems worldwide.
Biomarkers may play an important role in highlighting the presence, absence or severity of sepsis.
Materials and methods: This study is an retrospective study, performed on patients with suspected sepsis (81 patients) from a total of 10,483 patients who where presented themselves in the Emergency Department-"Sf. Spiridon" Hospital-Iasi between 01.09.2014-30.10.2014. The study aims was to establish the following aspects: determining the validity of presepsin as a biological diagnostic and prognostic marker of sepsis and mortality at 30 days after presentation moments in the Emergency Department.
Results: The mean age of patients was 64.52 years. Determination of presepsin sensitivity in early diagnosis of sepsis was calculated by generating the ROC curve, the AUC values (Area Under the Curve) obtained were: AUC=0.709, with a standard error of 0.065 for sepsis prediction; AUC=0.866, with a standard error of 0.080 for severe sepsis; AUC=0.864, with a standard error of 0.053 in the case of septic shock. The AUC calculated for presensin susceptibility to mortality was 0.764, with a standard error of 0.062.
Conclusion: Presepsin, determined by using quantitative dosing methods, can be of real use in the staging of patients diagnosed with sepsis, and may be indicative of initiating intensive care to prevent the onset of septic shock. Presepsin may be an early marker of mortality in the septic patient.
Presepsin: Early Biomarker in Diagnosis of Sepsis in Emergency Department Ovidiu Popa1, Diana Cimpoieșu1* and Carmen Dorobăț2
1Emergency Department, St. “Spiridon” Hospital Iași, “Gr. T. Popa” University of Medicine and Pharmacy, Iași, Romania2Department of Infectious Disease, Clinic Infectious Diseases Hospital Iași, “Gr. T. Popa” University of Medicine and Pharmacy, Iași, Romania
de răspuns inflamator sistemic din cadrul bolilor infecțioase bacteriene și nonbacteriene, a fost determinată la 600 pg/ml , cu o sensibilitatea de 87.8% și specificitate de 81.4% [3].
Material și MetodăStudiul este un studiu prospectiv, efectuat pe un lot de 81 de pacieți
cu suspiciune de sepsis dintr-un total de 10483 pacienți ce s-au prezentat în Unitatea Primire Urgențe-Spitalul Clinic Județean de Urgență “Sf. Spiridon”-Iași în perioada 01.08.2014-30.10.2014.
Studiul și-a prOpus să stabilească următoarele aspecte
Determinarea validității presepsinei ca marker biologic diagnostic și prognostic de sepsis; mortalitatea la 30 de zile de la prezentarea in Unitatea Primire Urgente.
Protocolul de studiu a cuprins pentru lotul de pacienți următoarele
date epidemiologice, variabile clinice și paraclinice, elementele de terapie administrată din momentul prezentării în Unitatea Primire Urgențe-Spitalul “Sf. Spiridon”-Iași, evoluție la 28 de zile.
Volume 13 • Issue 3 • 1J Surgery, an open access journalISSN: 1584-9341
Criterii de includere
Pacienți cu vârsta peste 18 ani. Pacienți cu semne clinice de infecție însoțită de prezența a cel puțin două din criteriile următoare: temperatură >38°C sau <36°C, frecvența cardiacă >90/min, frecvența respiratorie >20/min și leucocitoză (>12.000 mm3) sau leucopenie (<4000 mm3).
Criterii de excludere
Pacienții cu varsta sub 18 ani. Paciente gravide sau aflate în perioada de alăptare.
Diagnosticul de sepsis a fost pus pe baza tabloului clinic general coroborat cu investigațiile paraclinice, urmărindu-se criteriile de diagnostic statuate de Surviving Sepsis Campaign (4).
Pentru fiecare pacient cu suspiciune de sepsis abordarea în departamentul de urgență a fost standardizată pe baza protocoalelor specifice acestei specialități. Pacientul este evaluat clinic, se monitorizează funcțiile vitale și în momentul suspiciunii clinice de infectie s-a trecut la completarea unei fise de caz cuprinzand variabilele clinice si paraclinice menționate în definția sepsisului.
Datele colectate pentru din fisele pacientiilor care au întrunit criteriile de includere au fost prelucrate statistic, utilizând programul de analiză statistică IBM-SPSS v.22.
Rezultate Structural lotul de studiu a fost aproximativ egal distribuit în funcție
de sexul pacienților, se observă o ușoară predominanță a sexului feminin (51.85%). Statistic se evidențiază o vârstă medie a participanților la studiu de 64,52 ani, cu o deviație standard de 15.36 ani.
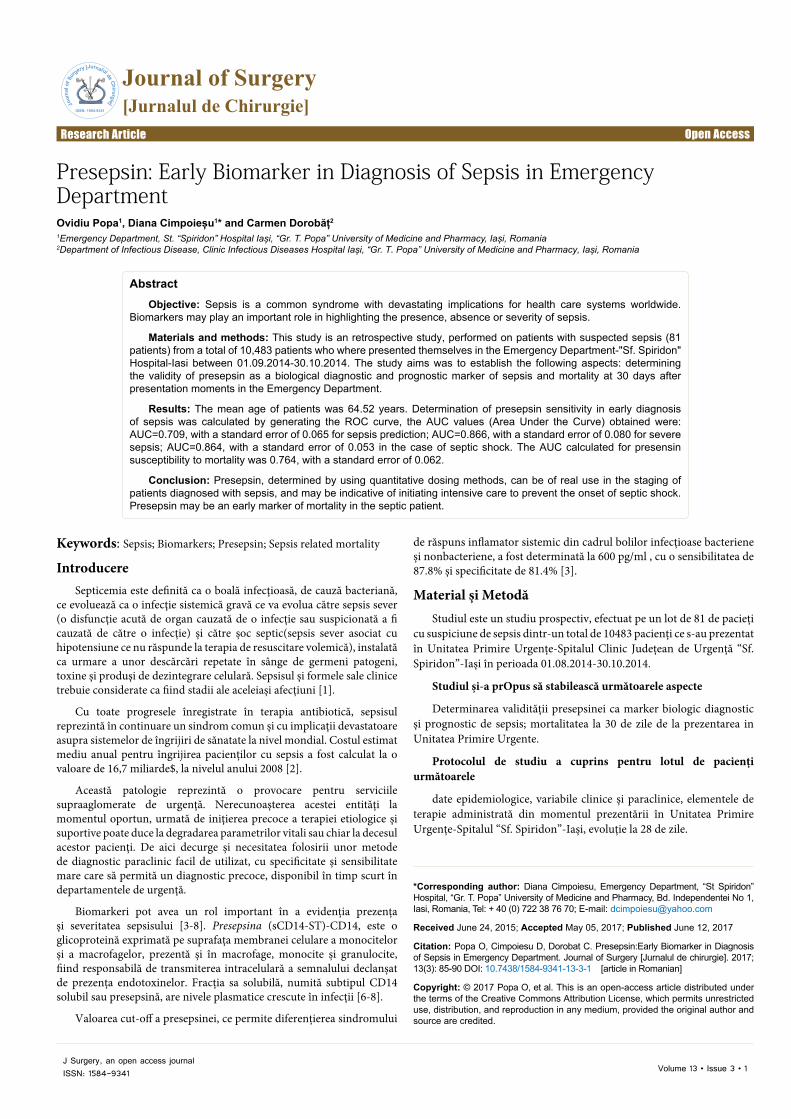
Din totalul pacienților prezentați și incluși în studiul de față, un număr de 27 dintre aceștia, corespunzător unui procent de 33.33% au fost diagnosticați după finalizarea tuturor investigațiilor clinice și paraclinice cu diagnosticul de sepsis, aici fiind incluși pacienții cu sepsis, sepsis sever și șoc septic, restul prezentând SIRS sau infecții simple (Figura 1).
Am înregistrat în lotul de pacienți prezența antecedentelor patologice cardio-vasculare, pulmonare, endocrine, gastro-intestinale, neurologice, renale, inclusiv sepsis în antecedente, pentru a verifica dacă există o posibilă corelație între existența acestora și diagnosticul de sepsis prezent. De menționat că dintre antecedentele personale patologice prezente la pacienții din lotul de studiu cele mai frecvent întâlnite au fost hipertensiunea arterială (24.69%), alte boli cardiovasculare (34.57%) și bolile endocrine (33.33%), categorie în care a fost inclus și diabetul zaharat.
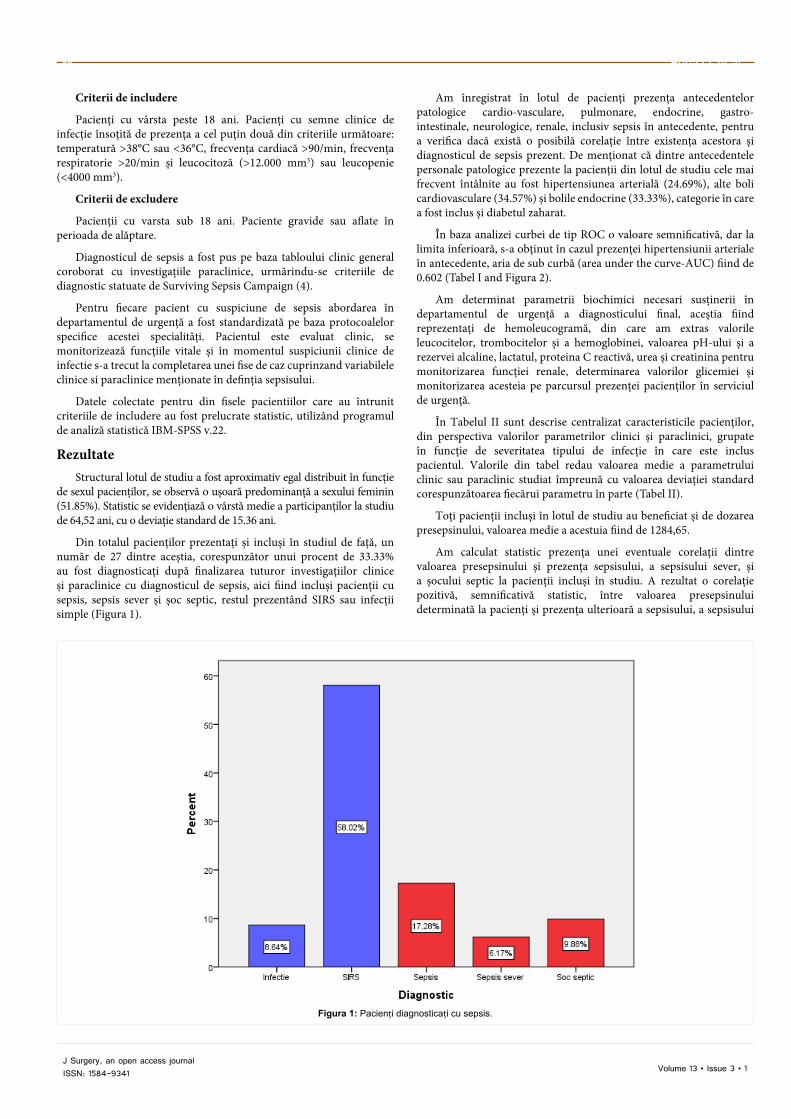
În baza analizei curbei de tip ROC o valoare semnificativă, dar la limita inferioară, s-a obținut în cazul prezenței hipertensiunii arteriale în antecedente, aria de sub curbă (area under the curve-AUC) fiind de 0.602 (Tabel I and Figura 2).
Am determinat parametrii biochimici necesari susținerii în departamentul de urgență a diagnosticului final, aceștia fiind reprezentați de hemoleucogramă, din care am extras valorile leucocitelor, trombocitelor și a hemoglobinei, valoarea pH-ului și a rezervei alcaline, lactatul, proteina C reactivă, urea și creatinina pentru monitorizarea funcției renale, determinarea valorilor glicemiei și monitorizarea acesteia pe parcursul prezenței pacienților în serviciul de urgență.
În Tabelul II sunt descrise centralizat caracteristicile pacienților, din perspectiva valorilor parametrilor clinici și paraclinici, grupate în funcție de severitatea tipului de infecție în care este inclus pacientul. Valorile din tabel redau valoarea medie a parametrului clinic sau paraclinic studiat împreună cu valoarea deviației standard corespunzătoarea fiecărui parametru în parte (Tabel II).
Toți pacienții incluși în lotul de studiu au beneficiat și de dozarea presepsinului, valoarea medie a acestuia fiind de 1284,65.
Am calculat statistic prezența unei eventuale corelații dintre valoarea presepsinului și prezența sepsisului, a sepsisului sever, și a șocului septic la pacienții incluși în studiu. A rezultat o corelație pozitivă, semnificativă statistic, între valoarea presepsinului determinată la pacienți și prezența ulterioară a sepsisului, a sepsisului
Figura 1: Pacienți diagnosticați cu sepsis.
Presepsin-Early Biomarker 87
Volume 13 • Issue 3 • 1J Surgery, an open access journalISSN: 1584-9341
Test Result Variable(s) Area Std. Errora Asymptotic Sig.bAsymptotic 95% Confidence Interval
Tabel II: Caracteristici clinice și paraclinice pacienți incluși în studio.
Figura 2: Curba ROC pentru antecedente corelate cu diagnosticul de sepsis.
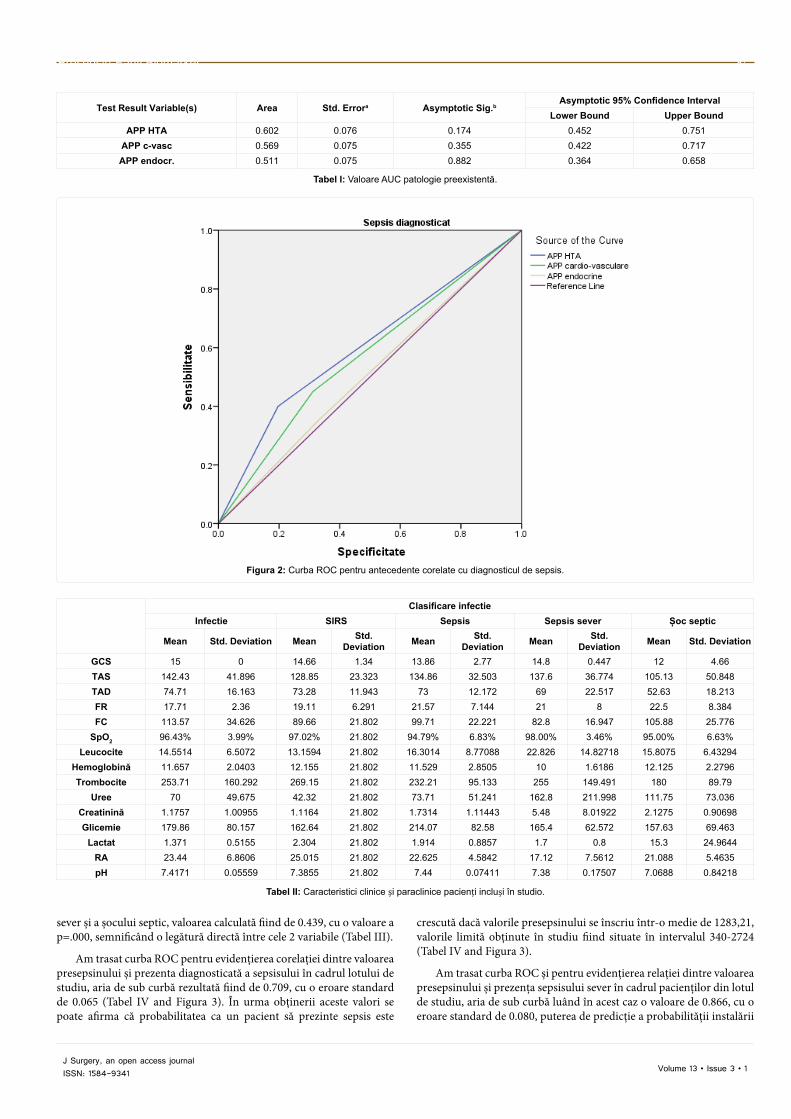
sever și a șocului septic, valoarea calculată fiind de 0.439, cu o valoare a p=.000, semnificând o legătură directă între cele 2 variabile (Tabel III).
Am trasat curba ROC pentru evidențierea corelației dintre valoarea presepsinului și prezenta diagnosticată a sepsisului în cadrul lotului de studiu, aria de sub curbă rezultată fiind de 0.709, cu o eroare standard de 0.065 (Tabel IV and Figura 3). În urma obținerii aceste valori se poate afirma că probabilitatea ca un pacient să prezinte sepsis este
crescută dacă valorile presepsinului se înscriu într-o medie de 1283,21, valorile limită obținute în studiu fiind situate în intervalul 340-2724 (Tabel IV and Figura 3).
Am trasat curba ROC și pentru evidențierea relației dintre valoarea presepsinului și prezența sepsisului sever în cadrul pacienților din lotul de studiu, aria de sub curbă luând în acest caz o valoare de 0.866, cu o eroare standard de 0.080, puterea de predicție a probabilității instalării
Popa O, et al.88
Volume 13 • Issue 3 • 1J Surgery, an open access journalISSN: 1584-9341
Tabel III: Corelatie valoare presepsin-sepsis.
Presepsin Sepsis diagnosticat
Sepsis diagnosticat
Pearson Correlation 0.439** 1
Sig. (2-tailed) 0.000
Covariance 463.718 0.225N 81 81
**Correlation is significant at the 0.01 level (2-tailed).
Area Std. Errora Asymptotic Sig.bAsymptotic 95% Confidence Interval
sepsisului în cazul unei valori medii de 4787,80 fiind mare (Tabel V and Figura 3).
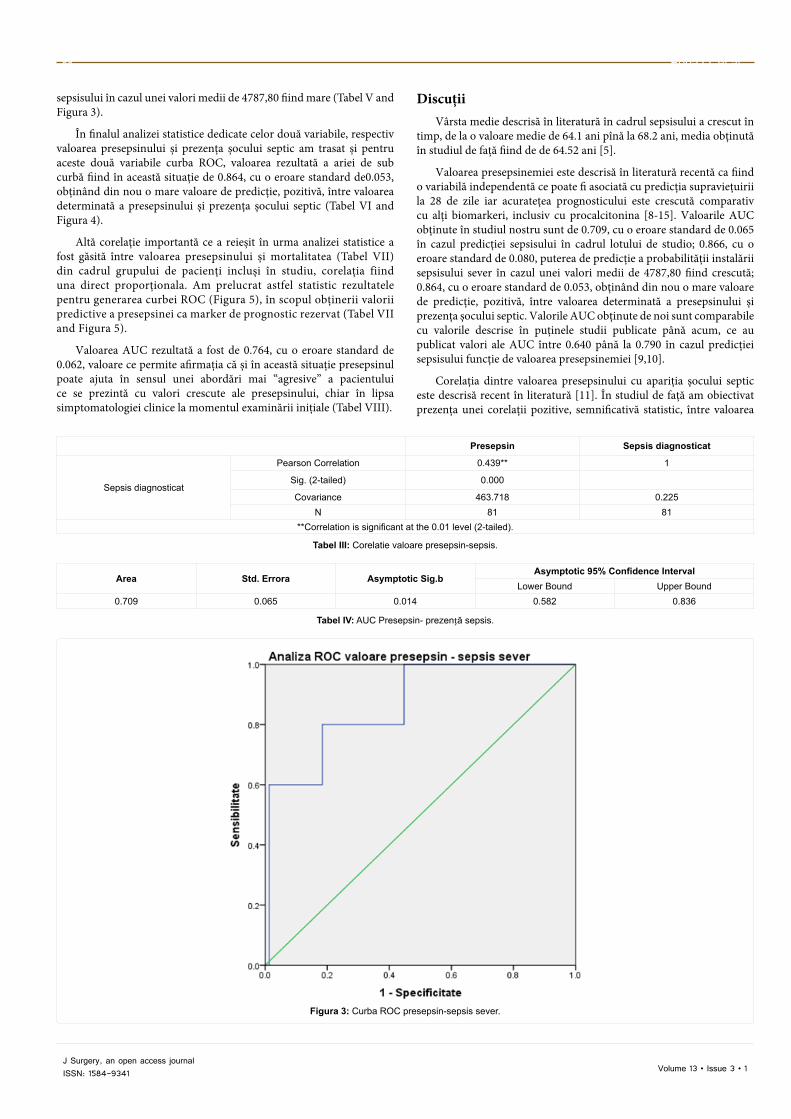
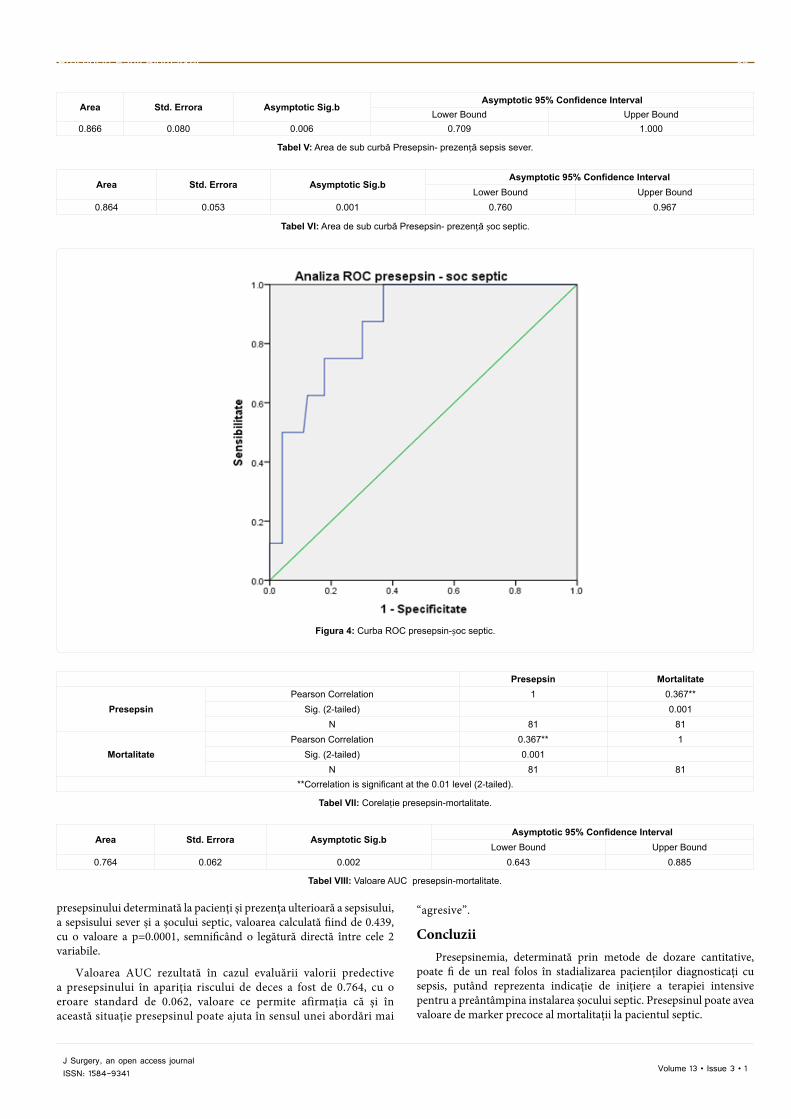
În finalul analizei statistice dedicate celor două variabile, respectiv valoarea presepsinului și prezența șocului septic am trasat și pentru aceste două variabile curba ROC, valoarea rezultată a ariei de sub curbă fiind în această situație de 0.864, cu o eroare standard de0.053, obținând din nou o mare valoare de predicție, pozitivă, între valoarea determinată a presepsinului și prezența șocului septic (Tabel VI and Figura 4).
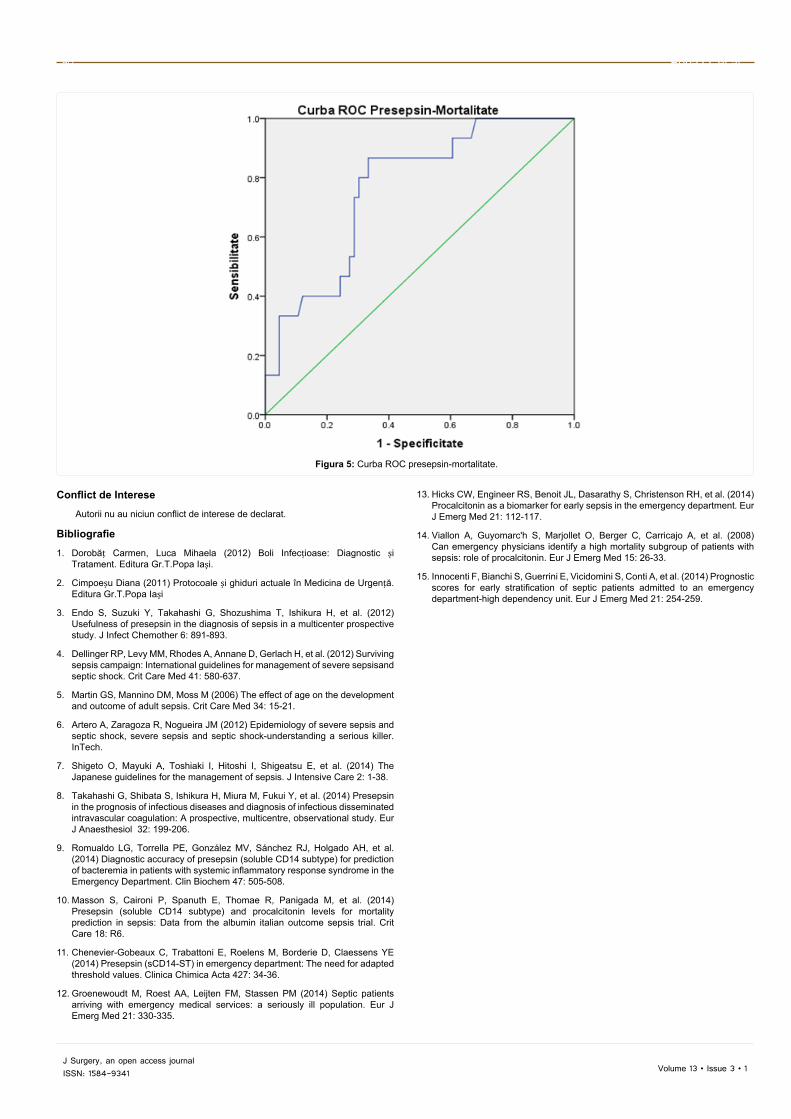
Altă corelație importantă ce a reieșit în urma analizei statistice a fost găsită între valoarea presepsinului și mortalitatea (Tabel VII) din cadrul grupului de pacienți incluși în studiu, corelația fiind una direct proporționala. Am prelucrat astfel statistic rezultatele pentru generarea curbei ROC (Figura 5), în scopul obținerii valorii predictive a presepsinei ca marker de prognostic rezervat (Tabel VII and Figura 5).
Valoarea AUC rezultată a fost de 0.764, cu o eroare standard de 0.062, valoare ce permite afirmația că și în această situație presepsinul poate ajuta în sensul unei abordări mai “agresive” a pacientului ce se prezintă cu valori crescute ale presepsinului, chiar în lipsa simptomatologiei clinice la momentul examinării inițiale (Tabel VIII).
DiscuțiiVârsta medie descrisă în literatură în cadrul sepsisului a crescut în
timp, de la o valoare medie de 64.1 ani pînă la 68.2 ani, media obținută în studiul de față fiind de de 64.52 ani [5].
Valoarea presepsinemiei este descrisă în literatură recentă ca fiind o variabilă independentă ce poate fi asociată cu predicția supraviețuirii la 28 de zile iar acuratețea prognosticului este crescută comparativ cu alți biomarkeri, inclusiv cu procalcitonina [8-15]. Valoarile AUC obținute în studiul nostru sunt de 0.709, cu o eroare standard de 0.065 în cazul predicției sepsisului în cadrul lotului de studio; 0.866, cu o eroare standard de 0.080, puterea de predicție a probabilității instalării sepsisului sever în cazul unei valori medii de 4787,80 fiind crescută; 0.864, cu o eroare standard de 0.053, obținând din nou o mare valoare de predicție, pozitivă, între valoarea determinată a presepsinului și prezența șocului septic. Valorile AUC obținute de noi sunt comparabile cu valorile descrise în puținele studii publicate până acum, ce au publicat valori ale AUC între 0.640 până la 0.790 în cazul predicției sepsisului funcție de valoarea presepsinemiei [9,10].
Corelația dintre valoarea presepsinului cu apariția șocului septic este descrisă recent în literatură [11]. În studiul de față am obiectivat prezența unei corelații pozitive, semnificativă statistic, între valoarea
Presepsin-Early Biomarker 89
Volume 13 • Issue 3 • 1J Surgery, an open access journalISSN: 1584-9341
Area Std. Errora Asymptotic Sig.bAsymptotic 95% Confidence Interval
presepsinului determinată la pacienți și prezența ulterioară a sepsisului, a sepsisului sever și a șocului septic, valoarea calculată fiind de 0.439, cu o valoare a p=0.0001, semnificând o legătură directă între cele 2 variabile.
Valoarea AUC rezultată în cazul evaluării valorii predective a presepsinului în apariția riscului de deces a fost de 0.764, cu o eroare standard de 0.062, valoare ce permite afirmația că și în această situație presepsinul poate ajuta în sensul unei abordări mai
“agresive”.
ConcluziiPresepsinemia, determinată prin metode de dozare cantitative,
poate fi de un real folos în stadializarea pacienților diagnosticați cu sepsis, putând reprezenta indicație de inițiere a terapiei intensive pentru a preântâmpina instalarea șocului septic. Presepsinul poate avea valoare de marker precoce al mortalitații la pacientul septic.
Popa O, et al.90
Volume 13 • Issue 3 • 1J Surgery, an open access journalISSN: 1584-9341
Figura 5: Curba ROC presepsin-mortalitate.
Conflict de Interese
Autorii nu au niciun conflict de interese de declarat.
Bibliografie
1. Dorobăț Carmen, Luca Mihaela (2012) Boli Infecțioase: Diagnostic și Tratament. Editura Gr.T.Popa Iași.
2. Cimpoeșu Diana (2011) Protocoale și ghiduri actuale în Medicina de Urgență. Editura Gr.T.Popa Iași
3. Endo S, Suzuki Y, Takahashi G, Shozushima T, Ishikura H, et al. (2012) Usefulness of presepsin in the diagnosis of sepsis in a multicenter prospective study. J Infect Chemother 6: 891-893.
4. Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, et al. (2012) Surviving sepsis campaign: International guidelines for management of severe sepsisand septic shock. Crit Care Med 41: 580-637.
5. Martin GS, Mannino DM, Moss M (2006) The effect of age on the development and outcome of adult sepsis. Crit Care Med 34: 15-21.
6. Artero A, Zaragoza R, Nogueira JM (2012) Epidemiology of severe sepsis and septic shock, severe sepsis and septic shock-understanding a serious killer. InTech.
7. Shigeto O, Mayuki A, Toshiaki I, Hitoshi I, Shigeatsu E, et al. (2014) The Japanese guidelines for the management of sepsis. J Intensive Care 2: 1-38.
8. Takahashi G, Shibata S, Ishikura H, Miura M, Fukui Y, et al. (2014) Presepsin in the prognosis of infectious diseases and diagnosis of infectious disseminated intravascular coagulation: A prospective, multicentre, observational study. Eur J Anaesthesiol 32: 199-206.
9. Romualdo LG, Torrella PE, González MV, Sánchez RJ, Holgado AH, et al. (2014) Diagnostic accuracy of presepsin (soluble CD14 subtype) for prediction of bacteremia in patients with systemic inflammatory response syndrome in the Emergency Department. Clin Biochem 47: 505-508.
10. Masson S, Caironi P, Spanuth E, Thomae R, Panigada M, et al. (2014) Presepsin (soluble CD14 subtype) and procalcitonin levels for mortality prediction in sepsis: Data from the albumin italian outcome sepsis trial. Crit Care 18: R6.
11. Chenevier-Gobeaux C, Trabattoni E, Roelens M, Borderie D, Claessens YE (2014) Presepsin (sCD14-ST) in emergency department: The need for adapted threshold values. Clinica Chimica Acta 427: 34-36.
12. Groenewoudt M, Roest AA, Leijten FM, Stassen PM (2014) Septic patients arriving with emergency medical services: a seriously ill population. Eur J Emerg Med 21: 330-335.
13. Hicks CW, Engineer RS, Benoit JL, Dasarathy S, Christenson RH, et al. (2014) Procalcitonin as a biomarker for early sepsis in the emergency department. Eur J Emerg Med 21: 112-117.
14. Viallon A, Guyomarc'h S, Marjollet O, Berger C, Carricajo A, et al. (2008) Can emergency physicians identify a high mortality subgroup of patients with sepsis: role of procalcitonin. Eur J Emerg Med 15: 26-33.
15. Innocenti F, Bianchi S, Guerrini E, Vicidomini S, Conti A, et al. (2014) Prognostic scores for early stratification of septic patients admitted to an emergency department-high dependency unit. Eur J Emerg Med 21: 254-259.
IntroductionColorectal cancer is one of the most commonly diagnosed cancers
worldwide. Its incidence increases with age and higher mortality rate is encountered in men [1]. Therapeutic approach refers to a complex surgical, chemo-and radiotherapy treatment.
In spite of numerous surgical techniques developed in the last decades-including new mechanical stapler based methods-anastomotic leakage (AL) remains one of the most feared complications in colorectal surgery. Its incidence ranges from 1.5% to 16% for “per primam” anastomoses with frequent need for redo interventions, longer hospitalization and high mortality rates [2]. AL prediction and identification are still difficult due to its different clinical manifestations, varying from vague abdominal symptoms and prolonged postoperative ileus to fulminant abdominal pain in case of peritonitis and sepsis [3]. It is still a challenging task to distinguish early after surgery the developing septic process from the physiological inflammatory response; however, early diagnosis, before the appearance of clinical symptoms, remains essential for a long term survival [4]. The literature recognizes several risk factors for AL development such as diabetes, smoking, obesity, chronic kidney disease, cardiovascular diseases but facts are still contradictory [5-7]. According to several authors [8,9] characteristics of AL depend on many aspects:
-The direction of the leakage has a major impact on the patient’s symptoms; internal leakages are drained to organs such as the vagina, gallbladder or bladder and external leakages are drained through the teguments.
*Corresponding author: Radu Micea Neagoe, University of Medicine and Pharmacy of Târgu Mureș, 2nd Department of Surgery, Emergency Mureș County Hospital, Târgu Mureș, Romania, Tel: +40 (0) 652 12 11 12 73; E-mail: [email protected]
Received July 28, 2017; Accepted August 15, 2017; Published August 22, 2017
Citation: Popescu G, Sala D, Gliga M, Ciulic S, Neagoe RM, et al. The Incidence and Mortality of Anastomotic Leakage after Colorectal Cancer Surgery. Journal of Surgery [Jurnalul de chirurgie]. 2017; 13(3): 91-93 DOI: 10.7438/1584-9341-13-3-2
AbstractIntroduction: Anastomotic leakage (AL) remains one of the most feared complications after colorectal surgery
with high mortality rates, prolonged hospitalization, highly risk of readmission, finally generating important costs for any healthcare system. AL prediction and early detection are a considerable challenge for each surgeon as no well-established and reliable predictors and diagnosis protocols are currently available.
Aims: To determine the incidence and mortality of AL after colorectal surgery, with identification of possible predictors and improvement points in the management of this complication.
Material and methods: We included 431 patients with colorectal cancer who underwent surgical resection and restoration of the digestive tube’s continuity, at the 2nd Department of Surgery, Emergency County Clinical Hospital of Târgu-Mureș, from January 2010-December 2015. The patients have been divided in two groups: AL group including 21 patients and no leak group with 410 patients. Demographic characteristics and comorbidities were recorded with clinical and laboratory follow-up in the postoperative period.
Results: There were no significant differences between the two groups in terms of demographic characteristics and comorbidities. The average age of patients with AL was 65.9 ± 11.6 vs. 65.0 ± 10.3 without AL. Male gender was predominant in both groups. No significant differences were recorded in terms of the localization and type of intervention between the two groups. Elevated C reactive protein levels were significantly more frequent in patients with AL (p=0.03). The mortality rate in patients with AL was significantly higher compared to the no leak group 28.6% vs. 1.9% (p<0.0001).
Conclusions: AL remains the most feared complication in colorectal surgery, with high mortality rates, regardless of the localization of the anastomosis and type of intervention. Elevated C reactive protein levels may predict AL being helpful for the early detection and treatment of this complication.
The Incidence and Mortality of Anastomotic Leakage after Colorectal Cancer SurgeryGabriel Popescu1, Daniela Sala2, Miana Gliga1, Sergiu Ciulic1, Radu Mircea Neagoe1,2* and Mircea Mureșan1,2
1Department of Surgery II, Emergency Mureș County Hospital, Târgu Mureș, Romania2University of Medicine and Pharmacy of Târgu Mureș, Târgu Mureș, Romania
-AL’s may develop intra or extra peritoneal.
-Localizations of the AL may at the proximal or distal part of the anastomosis.
-The debit of the AL through the drain tube which could be small (<200 ml/24h), medium (200-500 ml/24h) or large (>500 ml/24 h).
-The severity of AL which might be minor (no clinical signs) or major (with clinical impact).
Numerous classifications are available, but no consensus exists over the medical world. The IMAGImE (International Multispecialty Anastomotic Leak Global Improvement Exchange) classification gives a simple clinical categorization of AL. Type A-with no or minimal clinical involvement, which does not need any active therapeutic intervention, Type B-which requires active treatment, but not surgical intervention and Type C-requiring surgical treatment [10].
Volume 13 • Issue 3 • 2J Surgery, an open access journalISSN: 1584-9341
This study aims to determine the incidence and mortality of AL after both elective and emergency procedures; we analyze possible AL’s predictors trying to identify improvement points in the management of this complication.
Material and MethodsIn our study the clinical and operative charts (2nd Department of
Surgery II, Emergency Mures County Hospital) were retrospectively analyzed between January 2010 and December 2015. We included 431 patients with colorectal cancer for whom surgical resection was performed with “per primam intentionem” restoration of the digestive tube’s continuity. The group of patients who developed AL was comparatively analyzed with those who did not exhibit this complication. Demographic characteristics and comorbidities of both groups were recorded; the type of surgical intervention, the localization and type of the anastomosis and the in-hospital mortality was determined for both groups. Patients with derivative surgical procedures were excluded, even if a later anastomosis was performed. No distinction was made between the types of procedures (manual or mechanical, continuous or separate sutures). Preoperative work-up included prophylactic antibiotherapy, cardiology and pre-anesthesia examinations. The postoperative follow-up and diagnosis of AL was based on clinical signs (fever, ileus, abdominal pain, altered state of the patient), laboratory examinations (total blood count, urea, creatinine, procalcitonin, C reactive protein) and imaging studies (abdominal echography, abdominal computed tomography), according to local protocols. The study was approved by ethical commission of the institution and it was realized in accordance with ethical code of the Declaration of Helsinki.
Statistical Analysis Statistical analysis was carried out using the SPSS for Windows (v
20.0, IBM Corporation, Armonk, NY, USA) software program. The Kolmogorov-Smirnov test was used to assess the normal distribution of continuous numerical variables. The results were presented as numbers and percentages for qualitative variables and as average ± standard deviation or median values for quantitative variables. Facts were compared using Student test (for quantitative variables) and χ2 test (for qualitative variables). A value of p<0.05 was considered statistically significant.
ResultsAmong 431 patients included 21 (4.9%) were identified with
anastomotic leakage during hospitalization. All leakages were type C and needed surgical treatment. Primary emergency operation was performed for 1 patient (4.8%) from the group AL and for 33 patients (8%) in the group without AL (p=0.25). The average time to AL diagnosis was 6 days after the operation, with the earliest diagnosis on day 5th and the latest on day 13th. There was no significant difference between groups as regards demographic characteristics, associated comorbidities and risk factors such as diabetes, cardiovascular diseases, chronic kidney disease and obesity. The average age of patients with AL was 65.9 ± 11.6 vs. 65.0 ± 10.3 in the comparative group. Male gender was predominant in both groups, but with no significant difference between the two groups (Table I).
The majority of the tumors were localized at the level of the left colon (vascularized by the inferior mesenteric artery), with no significant difference between groups-42.8% in patients with AL vs. 38.8%, p=0.89. This location was followed by right colon tumors (vascularized by the superior mesenteric artery) with 28.6% (n=6) in the AL groups vs. 34.9%, p=0.72. No significant difference was observed in the incidence of rectal tumors between the two groups with 28.6% (n=60) in the AL group vs. 26.3% (n=108) in the no leak group (p=0.98). No significant differences were observed as concerned
the type of intervention; right hemicolectomy was most frequently performed in both groups (33.3% in the leak group vs. 36.4% in no leak group, p=0.94), followed by rectosigmoid resections (28.6% vs. 26.6%, p=0.95). Segmental colon resection of the colon was more often performed in the group with no leaks, but no significant difference was recorded (p=0.92). No left hemicolectomies and total colectomies were carried out in the anastomotic leak group. The type of anastomosis was identical in both groups, as proximal anastomoses (performed on the right colon) were more frequent than distal (performed on the left colon) ones (Table II).
The mortality rate was significantly higher in patients with AL compared to the no leak group (28.6% vs. 1.9%, p<0.0001). The average age of the deceased patients was 72 ± 12.52 years vs. 65 ± 10.37 years in the survivors of the AL group (p=0.11). There were no significant differences recorded in terms of the above-mentioned risk factors and comorbidities. Elevated C reactive protein levels (>5% over the accepted normal levels at the local laboratory) were significantly more frequently recorded in patients from the AL compared to the no leak group 85.71% (n=18) vs. 62.68% (n=257), (p=0.03).
DiscussionAnastomotic leaks still represent a major complication of colorectal
surgery; however, no particular risk factors have been yet identified. It has been shown that male gender, smoking, obesity, and diabetes might represent risk factors for AL, due to the vulnerability of these patients [11]; none of these were associated with higher incidence of AL in our study. Furthermore, the location of the tumor and anastomosis along with the type of intervention and surgical technique might also influence the development of AL [12]; in the current study no certain location or type of intervention proved to influence the AL’s appearance.
Usually AL is diagnosed between day 5th and 8th after the surgical intervention, those from first days being commonly associated with technical errors during surgery [13]. Early detection of this complication, thus avoiding a major peritonitis, is essential for the long-term survival of these patients [14]; in our study the average time of AL diagnosis was 6 days. Den Dulk at al. [15] proposed a clinical score for early detection of AL, so called “Dutch Leakage Score”, which analyzes different clinical and laboratory parameters. General vital signs such as fever (1 point), tachycardia (1 point), respiration frequency over 30/minute (1 point), diuresis-under 700ml/day or 30ml/hour (1 point), psychical-agitation or lethargy-and altered general state of the patient (1 point) along with local symptoms such as ileus, gastric stasis, evisceration or abdominal pain (2 points) are included. Laboratory parameters such as leukocytosis, elevated C reactive protein, creatinine, urea levels and parenteral feeding (1 point) are also part of the scoring system. The authors claimed that no diagnostic or therapeutic actions are needed ≤ 3 point; between 4-7 points severe monitoring is recommended and over 8 points contrast computed tomography is needed for diagnosis. This, yet not widely used score, might represent a useful tool in the early diagnosis of anastomotic leaks.
Anastomotic leaks detection, prior to the onset of clinical symptoms, is of paramount importance for better outcomes. In this
Anastomotic Leakage after Colorectal Cancer Surgery 93
Volume 13 • Issue 3 • 2J Surgery, an open access journalISSN: 1584-9341
perspective biomarkers could represent an objective indicator of the inflammatory process as a pathogenic substrate for AL development [16]. In a systematic review Su’a et al. [17] stated that systemic and peritoneal drainage fluid biomarkers cannot accurately predict the appearance of AL, but recommends the combination of these biomarkers for better results. In a recent study Smith et al. [18] defined the trajectory of C reactive protein as a possible gold standard biomarker for identification of anastomotic leaks after colorectal surgery. Our results also suggested that elevated C reactive proteins were significantly more frequently recorded in patients with AL than in the group without leakage.
The mortality rate after AL is high due to peritonitis with intense systemic inflammatory response and sepsis finally leading to multiple organ dysfunction or failure and death [19]. In our study, the mortality rate of patients with AL was highly significant in comparison with those who didn’t present this complication. Higher mortality rates are recorded in elderly patients who develop AL as a reason of cumulative comorbidities and frail immune system [11]. In our study, the deceased patients were older than the survivors, but no significant differences were observed.
ConclusionAnastomotic leaks still represent one of the major complications of
colorectal surgery with high mortality rates regardless of the localization of the anastomosis or the type of intervention. Elevated C reactive protein levels might predict the appearance of this complication, thus facilitating an early diagnosis. Early detection and proper treatment remains a great challenge for every surgeon, because any delay in this process has a major impact on the survival of these patients with longer hospitalization and higher costs. Application of a score system which includes clinical, laboratory and imagistic parameters, along with detection of new risk factors should be useful for the reduction of the mortality of this feared complication.
Conflict of Interest
Authors have no conflict of interest to disclose.
References
1. Haggar FA, Boushey RP (2009) Colorectal cancer epidemiology: Incidence, mortality, survival, and risk factors. Clin Colon Rectal Surg 22: 191-197.
2. Hammond J, Lim S, Wan Y, Gao X, Patkar A (2014) The burden of gastrointestinal anastomotic leaks: an evaluation of clinical and economic outcomes. J Gastrointest Surg 18: 1176-1185.
3. Khan AA, Wheeler JM, Cunningham C, George B, Kettlewell M, et al. (2008) The management and outcome of anastomotic leaks in colorectal surgery. Colorectal Dis 10: 587-592.
4. Welsh T, von Frankenberg M, Schmidt J, Büchler MW (2011) Diagnosis and definition of anastomotic leakage from surgeon's perspective. Chirurg 82: 48-55.
5. Slim K, Joris J, Beloeil H (2016) Colonic anastomosis and nonsteroidal antiinflammatory drugs. J Visc Surg 153: 269-275.
6. Parthasarathy M, Greensmith M, Bowers D, Groot-Wassink T (2016) Risk factors for anastomotic leakage after colorectal resection: a retrospective analysis of 17518 patients. Colorectal Dis 19: 288-29.
7. Dekker JW, Liefers GJ, de Mol van Otterloo JC, Putter H, Tollenaar RA (2011) Predicting the risk of anastomotic leakage in left-sided colorectal surgery using a colon leakage score. J Surg Res 166: e27-34.
8. Wang S, Liu J, Wang S, Zhao H, Ge S, et al. (2017) Adverse effects of anastomotic leakage on local recurrence and survival after curative anterior resection for rectal cancer: A systematic review and meta-analysis. World J Surg 41: 277-284.
9. Shogan BD, An GC, Schardey HM, Matthews JB, Umanskiy K, et al. (2014) Proceedings of the First International Summit on Intestinal Anastomotic Leak, Chicago, Illinois, 2012. Surg Infect (Larchmt) 15: 479-489.
10. Rahbari N, Weitz J, Hohenberger W, Heald RJ, Moran B, et al. (2010) Definition and grading of anastomotic leakage following anterior resection of the rectum: A proposal by the International Study Group of Rectal Cancer. Surgery 147: 339-351.
11. Rencuzogullari A, Benlice C, Valente M, Abbas MA, Remzi FH, et al. (2017) Predictors of anastomotic leak in elderly patients after colectomy: Nomogram-based assessment from the American College of Surgeons National Surgical Quality Program Procedure-Targeted Cohort. Dis Colon Rectum 60: 527-536.
12. Slieker JS, Daams F, Mulder IM, Jeekel J, Lange JF (2013) Systematic review of the technique of colorectal anastomosis. JAMA Surg 148: 190-201.
13. Feo LJ, Jrebi N, Asgeirsson T, Dujovny N, Figg R, et al. (2014) Anastomotic leaks: Technique and timing of detection. Am J Surg 207: 371-374.
14. Daams F, Wu Z, Cakir H, Karsten TM, Lange JF (2014) Identification of anastomotic leakage after colorectal surgery using microdialysis of the peritoneal cavity. Tech Coloproctol 18: 65-71.
15. den Dulk M, Witvliet MJ, Kortram K, Neijenhuis PA, de Hingh IH, et al. (2013) The DULK (Dutch Leakage) and modified DULK score compared: actively seek the leak. Colorectal Dis 15: 528-533.
16. Fraccalvieri D, Biondo S, Saez J, Millan M, Kreisler E, et al. (2012) Management of colorectal anastomotic leakage: differences between salvage and anastomotic takedown. Am J Surg 204: 671-676.
17. Su'a BU, Mikaere HL, Rahiri JL, Bissett IB, Hill AG (2017) Systematic review of the role of biomarkers in diagnosing anastomotic leakage following colorectal surgery. Br J Surg 104: 503-512.
18. Smith SR, Pockney P, Holmes R, Doig F, Attia J, et al. (2017) Biomarkers and anastomotic leakage in colorectal surgery: C-reactive protein trajectory is the gold standard. ANZ J Surg.
19. Rickert A, Willeke F, Kienle P, Post S (2010) Management and outcome of anastomotic leakage after colonic surgery. Colorectal Dis 12: 216-223.
Volume 13 • Issue 3 • 3J Surgery, an open access journalISSN: 1584-9341
Keywords Gall bladder volvulus; Cholecystectomy; Torsion; Cholelithiasis
IntroductionGall bladder volvulus is a rare and difficult to diagnose clinically as
well radiologically was first described by Wendel in 1898 [1]. More than 400 cases are reported in literature [1,2]. Volvulus of gall bladder is more common in elderly females between 7th and 8th decades and female to male ratio of 3:1 [3]. Causes has been attributed to anatomical variations of gall bladder mesentry and loss of visceral fat, as well mesentery with cystic duct and artery known as floating gall bladder [4-7]. When there is strong peristaltic movement or when the stomach contracts, intestines may turn and curl the gall bladder. Morbidity and mortality reported are low among cases of gall bladder torsion that have been diagnosed and treated early [8]. Delayed or missed diagnosis and treatment increase patient mortality. Symptoms vary depending on severity of disease.
Although recent advance in radiology help to diagnose many diseases, abdominal computed tomography (CT) and ultrasonography (USG) remains non-specific in diagnosing volvulus of gall bladder. Coronal magnetic resonance imaging (MRI) and magnetic resonance colangio-pancreatography (MRCP) and HIDA (hepatoiminodiacetic acid) scan are helpful in making the diagnosis of volvulus of gall bladder. We report as case of gall bladder volvulus with cholelithiasis treated by laparoscopic cholecystectomy and review of gall bladder volvulus.
Case PresentationA 56 year old female reported in OPD with ultrasound diagnosis of
acute cholecystitis with cholelithiasis. Patient was having history of pain for last 2 days which was dull and was associated with vomiting.
Clinically patient was pyrexic with no acute distress with stable vital signs. Abdomen was soft, mildly distended and tenderness in right upper quadrant and a positive Murphy’s sign.
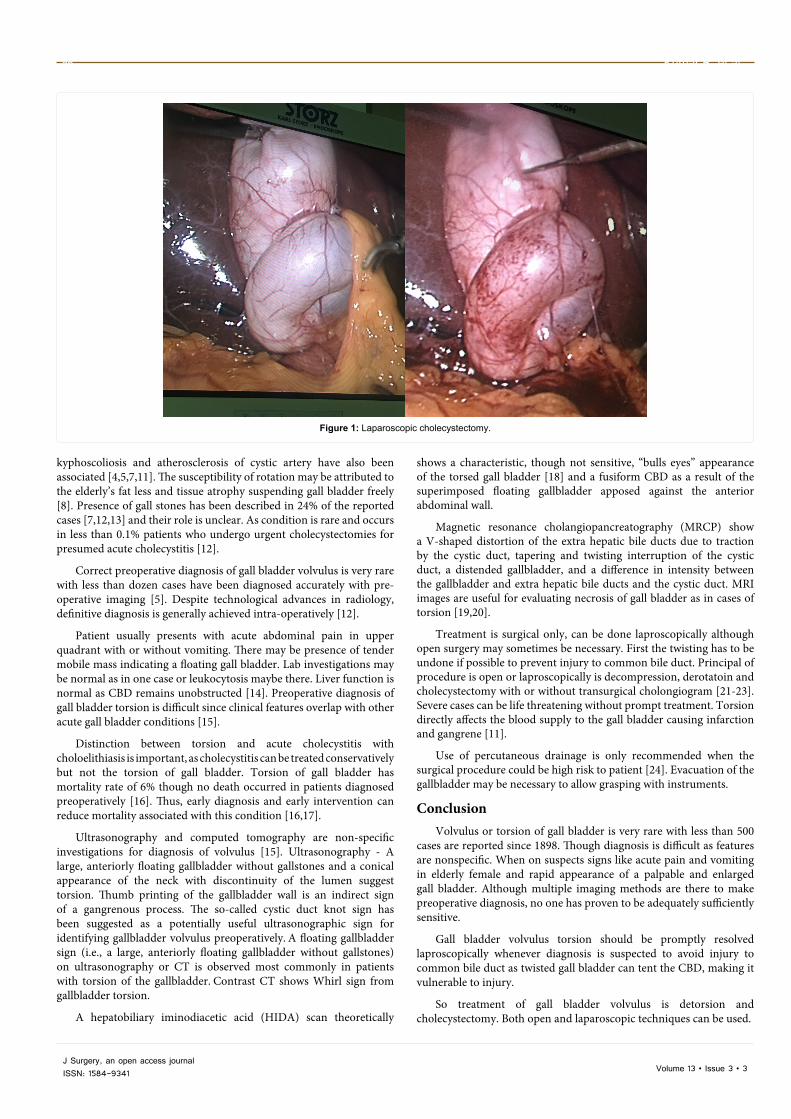
After routine investigations for laparoscopic cholecystectomy next day patient was taken up for surgery. Preoperative evaluation was unremarkable. On admission into operating room, patient was monitored with ECG, noninvasive blood pressure and pulse oximetre. Anasthesia was induced by 4.0 mg of midazolam and 5 mg of Scoline, muscles were paralyzed by 50 mg of atracurium. Endotracheal intubation 7.0 mm was placed into trachea to a depth of 20 cm from front teeth. Pure oxygen was used to mechanically ventilate the lungs. Laparoscopically we found distended rotated gall bladder with a complete mesentery which was large and allows the gallbladder to hang freely i.e., recognized situation 4 of gallbladder in relation to liver as discussed in detail in discussion. Surgery was uneventful after aspiration of clear fluid from gall bladder and derotation of gall bladder, laparoscopic cholecystectomy was done
*Corresponding author: Rajneesh Kumar, Department of Surgery, Punjab Institute of Medical Sciences [PIMS], Jalandhar, Punjab, India, Tel: 09814052513; 01812472688; E-mail: [email protected]
Received July 17, 2017; Accepted August 11, 2017; Published August 18, 2017
Citation: Kumar R, Hastir A, Walia RS. Volvulus of Gall Bladder -Case Report and Review of Literature. Journal of Surgery [Jurnalul de chirurgie]. 2017; 13(2): 95-97 DOI: 10.7438/1584-9341-13-3-3
AbstractGall bladder volvulus or twisting is a rare condition and occurs due to rotation of gall bladder. Preoperative
diagnosis is exception and usually misdiagnosed as cholecystitis before surgery. It is potentially fatal condition unless diagnosed and treated early leading to gangrene and biliary peritonitis. It has been reported in only about 500 cases in the literature ranging in age given 2-100 years old. We report a rare case of middle aged female 56 years old with volvulus of gall bladder having concomitant cholelithiasis treated with laparoscopic cholecystectomy.
Volvulus of Gall Bladder -Case Report and Review of LiteratureRajneesh Kumar*, Ankur Hastir and Ramandeep Singh WaliaDepartment of Surgery, Punjab Institute of Medical Sciences, Jalandhar, Punjab, India
taking care of cystic duct and artery. There were no abnormal findings in abdomen Patient discharged next day and stitches were removed after 8 days (Figure 1).
DiscussionGall bladder volvulus or twisting or torsion is a rare condition
primarily seen in elderly women, can be very painful and serious condition, requiring immediate surgical intervention. Complete twist leads to obscure blood flow and in due time there could be gangrene which is life threatening. Worst thing is there is no specific symptom of twisted gall bladder or gall bladder torsion.
First reported by Wendel in 1898 [1], Wendel described a configuration named the “Floating gall bladder” where gall bladder is pedunculated, hanging free of the liver and attached only by cystic mysentery. Volvulus of gall bladder is relatively uncommon condition with no more than 500 cases reported in literature [9]. Gall bladder volvulus or torsion, when gall bladder rotates either clockwise or anticlockwise around its mesentery along the axis of cystic duct and cystic artery causing complete obstruction of blood flow and biliary damage, resulting in acute gangrenous cholecystititis [3]. Anatomical variations of peritoneal covering of gall bladder are well known. There are five recognized positions of gall bladder in relation to liver.
• Completely embedded in liver.
• Closely attached to the under surface of the liver by the peritoneum.
• A complete mesentery but held closely to liver.
• A complete mesentery which is large and allows the gall bladder to hang freely.
• An incomplete mesentery which is attached along the cystic duct and allows gall bladder to hang freely in peritoneal cavity.
Only situations 4 and 5 can predispose to torsion of gall bladder [10]. Intense peristalsis of stomach, duodenum and colon as well as
Volume 13 • Issue 3 • 3J Surgery, an open access journalISSN: 1584-9341
Figure 1: Laparoscopic cholecystectomy.
kyphoscoliosis and atherosclerosis of cystic artery have also been associated [4,5,7,11]. The susceptibility of rotation may be attributed to the elderly’s fat less and tissue atrophy suspending gall bladder freely [8]. Presence of gall stones has been described in 24% of the reported cases [7,12,13] and their role is unclear. As condition is rare and occurs in less than 0.1% patients who undergo urgent cholecystectomies for presumed acute cholecystitis [12].
Correct preoperative diagnosis of gall bladder volvulus is very rare with less than dozen cases have been diagnosed accurately with pre-operative imaging [5]. Despite technological advances in radiology, definitive diagnosis is generally achieved intra-operatively [12].
Patient usually presents with acute abdominal pain in upper quadrant with or without vomiting. There may be presence of tender mobile mass indicating a floating gall bladder. Lab investigations may be normal as in one case or leukocytosis maybe there. Liver function is normal as CBD remains unobstructed [14]. Preoperative diagnosis of gall bladder torsion is difficult since clinical features overlap with other acute gall bladder conditions [15].
Distinction between torsion and acute cholecystitis with choloelithiasis is important, as cholecystitis can be treated conservatively but not the torsion of gall bladder. Torsion of gall bladder has mortality rate of 6% though no death occurred in patients diagnosed preoperatively [16]. Thus, early diagnosis and early intervention can reduce mortality associated with this condition [16,17].
Ultrasonography and computed tomography are non-specific investigations for diagnosis of volvulus [15]. Ultrasonography - A large, anteriorly floating gallbladder without gallstones and a conical appearance of the neck with discontinuity of the lumen suggest torsion. Thumb printing of the gallbladder wall is an indirect sign of a gangrenous process. The so-called cystic duct knot sign has been suggested as a potentially useful ultrasonographic sign for identifying gallbladder volvulus preoperatively. A floating gallbladder sign (i.e., a large, anteriorly floating gallbladder without gallstones) on ultrasonography or CT is observed most commonly in patients with torsion of the gallbladder. Contrast CT shows Whirl sign from gallbladder torsion.
A hepatobiliary iminodiacetic acid (HIDA) scan theoretically
shows a characteristic, though not sensitive, “bulls eyes” appearance of the torsed gall bladder [18] and a fusiform CBD as a result of the superimposed floating gallbladder apposed against the anterior abdominal wall.
Magnetic resonance cholangiopancreatography (MRCP) show a V-shaped distortion of the extra hepatic bile ducts due to traction by the cystic duct, tapering and twisting interruption of the cystic duct, a distended gallbladder, and a difference in intensity between the gallbladder and extra hepatic bile ducts and the cystic duct. MRI images are useful for evaluating necrosis of gall bladder as in cases of torsion [19,20].
Treatment is surgical only, can be done laproscopically although open surgery may sometimes be necessary. First the twisting has to be undone if possible to prevent injury to common bile duct. Principal of procedure is open or laproscopically is decompression, derotatoin and cholecystectomy with or without transurgical cholongiogram [21-23]. Severe cases can be life threatening without prompt treatment. Torsion directly affects the blood supply to the gall bladder causing infarction and gangrene [11].
Use of percutaneous drainage is only recommended when the surgical procedure could be high risk to patient [24]. Evacuation of the gallbladder may be necessary to allow grasping with instruments.
Conclusion Volvulus or torsion of gall bladder is very rare with less than 500
cases are reported since 1898. Though diagnosis is difficult as features are nonspecific. When on suspects signs like acute pain and vomiting in elderly female and rapid appearance of a palpable and enlarged gall bladder. Although multiple imaging methods are there to make preoperative diagnosis, no one has proven to be adequately sufficiently sensitive.
Gall bladder volvulus torsion should be promptly resolved laproscopically whenever diagnosis is suspected to avoid injury to common bile duct as twisted gall bladder can tent the CBD, making it vulnerable to injury.
So treatment of gall bladder volvulus is detorsion and cholecystectomy. Both open and laparoscopic techniques can be used.
Gall bladder volvulus 97
Volume 13 • Issue 3 • 3J Surgery, an open access journalISSN: 1584-9341
Conflict of Interest
There is no conflict of interest.
References
1. Wendel AV (1898) A case of floating gallbladder and kidney complicated with cholelithiasis with perforation of the gallbladder. Ann Surg 27: 199-202.
2. Reilly DJ, Kalogeropoulos G, Thiruchelvam D (2012) Torsion of the gallbladder: A systematic review. HPB 14(10): 669-672.
3. Mouawad NJ, Crofts B, Streu R, Desrochers R, Kimball BC (2011) Acute gallbladder torsion-a continued pre-operative diagnostic dilemma. World Journal of Emergency Surgery 6: 1-5.
4. Tarhan OR, Barut I, Dinelek H (2006) Gallbladder volvulus: Review of the literature and report of a case. Turk J Gastroenterol 17: 209-211.
5. Nicholas JM (2002) Image of the month: Gallbladder volvulus. Arch Surg 137: 741-742.
6. Stieber AC, Bauer JJ (1983) Volvulus of the gallbladder. Am J Gastroenterol 78: 96-98.
7. Chiow AKH, Ibrahim S, Tay KH (2007) Torsion of the gallbladder: A rare entity. Ann Acad Med Singapore 36: 705-706.
8. Shaikh AA, Charles A, Domingo S, Schaub G (2005) Gallbladder volvulus: report of two original cases and review of the literature. Am Surg 71: 87-89.
9. Pu TW, Fu CY, Lu HE, Cheng WT (2014) Complete body-neck torsion of the gallbladder: A case report. World J Gastroenterol 20: 14068-72.
10. Chilton CP, Mann CV (1980) Torsion of the gallbladder in a nine-year-old boy. J R Soc Med 73: 141-143.
11. Yeh HC, Weiss MF, Gerson CD (1989) Torsion of the gallbladder: The ultrasonographic features. J Clin Ultrasound 17: 123-125.
12. Nakao A, Matsuda T, Funabiki S, (1999) Gallbladder torsion: Case report and review of 245 cases reported in Japanese literature. J Hepatobiliary Pancreat Surg 6: 418-421.
13. Losken A, Wilson BW, Sherman R (1997) Torsion of the gallbladder: A case report and review of the literature. Am Surg 63: 975-978.
14. Garciavilla PC, Alvarez JF, Uzqueda GV (2010) Diagnosis and laparoscopic approach to gallbladder torsion and cholelithiasis. JSLS 14: 147-151.
15. Boonstra EA, Van Etten B, Prins TR, Sieders E, Van Leeuwen BL (2012) Torsion of the gallbladder. J Gastrointest Surg 16: 882-884.
16. Vedanayagam MS, Nikolopoulos I, Janakan G, El-Gaddal A (2013) Gallbladder volvulus: A case of mimicry. BMJ Case Reports, 2013.
17. Janakan G, Ayantunde AA, Hoque H (2008) Acute gallbladder torsion: An unexpected intraoperative finding. World Journal of Emergency Surgery.
18. Wang GJ, Colln M, Crossett J, Holmes RA (1987) Bulls-eye image of gallbladder volvulus. Clin Nucl Med 12: 231-232.
19. Fukuchi M, Nakazato K, Shoji H, Naitoh H, Kuwano H (2012) Torsion of the gallbladder diagnosed by magnetic resonance cholangiopancreatography. Int Surg 97: 235-238.
20. Usui M, Matsuda S, Suzuki H, Ogura Y (2000) Preoperative diagnosis of gallbladder torsion by magnetic resonance cholangiopancreatography. Scand J Gastroenterol 35: 218-222.
21. Reddy PK, Muralidharam M, Venkatasubram R (2005) Laparoscopic derotation and cholecystectomy for torsion gallbladder. JSLS 9: 238-240.
22. Amarillo HA, Pirchi ED, Mihura ME (2003) Complete gallbladder and cystic pedicle torsion: Laparoscopic diagnosis and treatment. Surg Endosc 17: 832-833.
23. Nguyen T, Geraci A, Bauer JJ (1995) Laparoscopic cholecystectomy for gallbladder volvulus. Surg Endosc 9: 519-521.
24. Bor-Gang Wu, Chao-Chuan Wu, Yao Jen Chang (2008) Torsion of the gallbladder. Surgery 143: 294-295.
IntroductionDuring the fifth to seventh week of gestation, midgut enlarges rapidly
and as it becomes too large for the abdominal cavity, it herniates through the umbilical cord. The apex of the herniated midgut is continuous with VID and yolk sac. Superior mesenteric artery forms the axis of this herniated midgut. Around tenth week of gestation herniated midgut returns back into the peritoneal cavity [1,2]. During this complex developmental process several anomalies may occur because of the complexity of the process. Examples include bowel atresias and stenoses, abnormalities of the vitellointestinal duct (Meckel's diverticulum, patent vitellointestinal duct (PVID), umbilical fistulas, umbilical sinus tracts, umbilical cysts and umbilical polyps), failure of ceacal descent, malrotation, malfixation, reversed bowel rotation and exomphalos [1-3]. VID is more common in males and mostly presents in first 28 days of life. This anomaly needs to be managed urgently to prevent gangrene.
Case PresentationA male neonate delivered via LSCS (CAUSE- PREVIOUS LSCS)
which was unbooked delivery 34 weeks with LMP-3/12/16 and EDD-10/9/17 WITH G4P3L3A1 was admitted in Yashoda Hospital, Ghazaibad, U.P. Baby was born at preterm. Antenatal scans were reported to be abnormal showing anterior wall depressed-pouch and part of intestine coming out from umbilicus. Birth weight was 2250 g and Apgar scores were 8/1, 9/1, 10/10. On examination at birth, new-born was having respiratory distress and grunting, so oxygen was started immediately and chest x-ray and arterial blood gas (ABG) was done. Chest x-ray showed grade 2 Hyaline Membrane Disease (HMD) and ABG showed respiratory acidosis, for which child was intubated and ventilated, also received surfactant. Abdominal examination revealed a bright red ‘Y’ shaped loop of small intestine was protruding from the umbilical ring. It was fixed to the umbilicus, with easily bleeding mucosa and irreducibility. Rest of the abdomen was not distended non tender (Figures 1 and 2). Bowel sounds were absent. There was no bilious aspirate in the orogastric tube. Anal opening was normally placed and patent, however, he had not passed any meconium. Patient had passed clear urine twice and the bladder was not palpable. Rest of the systemic examination was normal.
*Corresponding author: Karan Raheja, Pediatric Intensivist and Head of PICU, Yashoda hospital, Ghaziabad, Uttar Pradesh, India, Tel: +919899311517; E-mail: [email protected]
Received September 11, 2017; Accepted September 27, 2017; Published October 04, 2017
Citation: Raheja K, Aggarwal R, Prakash A, Kumar A, Sharma H, et al. Patent Vitellointestinal Duct with Inverted Ileal Loop Prolapse with Strangulation at Birth in Preterm (34 Weeks): A Rare Presentation. Journal of Surgery [Jurnalul de chirurgie]. 2017; 13(3): 99-100 DOI: 10.7438/1584-9341-13-3-4
AbstractPatent vitellointestinal duct (VID) can present to us in many variety of congenital intestinal malformations. Patient
presents with either anomaly alone or complications secondary to the anomaly. Most common reported anomaly of residual vitelline duct is Meckel’s diverticulum with different presentations like bleeding, intestinal obstruction or diverticulitis. Prolapsed ileal loops through a patent VID is a rare presentation of the above. To date only fifteen cases of this presentation have been reported in the English medical literature but none reported in a premature newborn baby presenting with it from the time of birth, which to the best of our knowledge has not been reported before and therefore this the youngest reported case of its nature in the current English medical literature.
Patent Vitellointestinal Duct with Inverted Ileal Loop Prolapse with Strangulation at Birth in Preterm (34 Weeks): A Rare PresentationKaran Raheja1*, Rajeev Aggarwal2, Ashish Prakash3, Arun Kumar4, Himanshu Sharma3 and Preeti Gupta5
Laboratory investigation including full hemogram, biochemistry and coagulation profile was normal. The newborn was started on intravenous fluids, antibiotics intravenous ceotaxim (100 mg/kg/day) and amikacin (15 mg/kg/day) and intramuscular vitamin K, 1 mg. Pediatric surgeon opinion was taken and patient was prepared for an emergency laparotomy because of the prolapsed ileal loops. Examination under anaesthesia revealed that prolapsed bowel loops, so patent VID was resected and end to end anastamosis was done in 2 layers and patient shifted to NICU. Baby was extubated successfully after 2 hours of surgery and remained haemodynamically stable. Baby was started on TPN as baby was kept NPO. On day-2 of admission child had abdominal distension with bilious aspirates along with no stools
Volume 13 • Issue 3 • 4J Surgery, an open access journalISSN: 1584-9341
passed till then. So, baby received enema of normal saline 5ml twice daily for next 3 days, after which baby passed stools and abdominal distension settled and was started on feeds. Feeds were gradually increased and TPN was tapered off and stopped. On day 10 of hospital stay child was discharged from the hospital.
DiscussionVitellointestinal duct (VID) or Omphalomesenteric duct connecting
the primitive gut to the yolk sac usually obliterates around the seventh or eighth week of gestation. Failure to obliterate may lead to variety of congenital anomalies including; Meckel's diverticulum, vitelline cord, umbilical sinus, enteric fistula and or haemorrhagic umbilical mass [1-4]. To date only 15 cases have been reported in the English medical literature [5-15]. Moreover, to the best of our knowledge there is no reported case of a new born presenting with patent VID with prolapsed (intussusceptions) of proximal and distal ileal loop. Antenatal diagnosis of a PVID anomaly can be confused with hernia of the umbilical cord or exomphalos minor which fails to obliterate on serial ultrasonography. Early diagnosis of PVID anomalies mandates surgeons to have a high index of suspicion in suspected cases. This would lead to prompt diagnosis and management of this rarity and save the neonate the morbidity and mortality associated with subsequent intestinal obstruction and ischemia. As noted in the previous case reports on the topic [1,2,15], outcome is highly dependent on time of presentation, early diagnosis, associated anomalies and the size of defect. When patients present late the approach must be more conservative with formal laparotomy and or ileostomies. However, if patients present early a trans-umbilical approach can be taken comfortably with good outcomes. Clinicians’ especially general practitioners need to be varying of a possible VID malformation in susceptible neonates when they present with intermittent discharge from the umbilicus. It is the widely patent type of PVID which are more likely to present with either complete or partial prolapse of ileum through the defect. The prolapse itself is probably caused by a sudden increase in intra-abdominal pressure associated with straining in neonates with a widely patent VID. Moreover, since the distance between the ileocecal valve and VID is shorter in neonates it leads to higher intraluminal pressure
causing double intussusception [14]. Resection and anastomosis is preferable to wedge resection of PVID because of the associated risk of ectopic gastric or pancreatic mucosa as well as the associated ischemia secondary to intestinal obstruction and strangulation [16]. We believe that this is a neonatal emergency which must be dealt with urgently due to the associated intestinal obstruction from intussusception, strangulation and gangrene of the prolapsed intestinal loop. In our case, we were able to do a primary closure of the VID following reduction of the prolapse due to the early presentation of the patient. All reported cases before this presented during late neonatal period or infancy. This patient however, presented with it from the time of birth, which makes us wonder whether perinatal events lead to its earlier presentation or was it a prenatal event. Therefore, clinician must have a very high index of suspicion for diagnosing it timely, though its management will always follow principals of standard neonatal bowel surgery.
ConclusionPatent vitellointestinal duct with prolapsed (intussusceptions) of
both proximal and distal ileal loop is a very rare occurrence together with being a neonatal surgical emergency due to the associated morbidity.
Acknowledgment
Consent for publication obtained from the parents of the patient.
References
1. Mohite PN, Bhatnagar AM, Hathila VP, Mistry JH (2007) Patent vitellointestinal duct with prolapse of inverted loop of small intestine: A case report. J Med Case Rep 1: 49.
2. Zea M, Chana R, Anees A, Khan S (2008) Inverted ileal prolapse through patent vitellointestinal duct: A case report. Internet J Pediatr Neonatol 10: 72-74.
3. Stone PA, Hofeldt MJ, Campbell JE, Vedula G, DeLuca JA, et al. (2004) Meckel diverticulum: Ten-year experience in adults. South Med J 97: 1038-1041.
4. Cullen JJ, Kelly KA, Moir CR, Hodge DO, Zinsmeister AR, et al. (1994) Surgical management of Meckel's diverticulum: An epidemiologic, population-based study. Ann Surg 220: 564-569.
5. Elebute EA, Ransome-Kuti O (1965) Patent vitello-intestinal duct with ileal prolapse. Arch Surg 91: 456-60.
6. Davis RM, Kehm RW (1967). Omphalocele with patent vitellointestinal duct and ileal prolapse. Am J Surg 113: 571-573.
7. Lal MM, Dhall JC (1976) Ileal prolapse through patent vitello-intestinal duct: A report of 3 cases with review of literature. Indian Pediatr 13: 571-573.
8. Rohatgi M, Gorthi SN (1984) Omphalocele with patent omphalomesenteric duct and ileal prolapse. Indian J Pediatr 51: 119-123.
9. Gvalani AK, Acharya AG, Rao RV (1985) Ileal prolapsed through a patent vitellointestinal. Indian Pr 38: 629-632.
10. Agrawal S, Memon A (2010) Patent vitellointestinal duct. BMJ Case Rep.
11. Singh S, Pandey A, Ahmed I, Rawat JD, Sharma A, et al. (2011) Prolapse of bowel via patent vitello intestinal ductda rare occurrence. Hernia 15: 567-569.
12. Pauleau G, Commandeur D, Andro C (2012) Intestinal prolapse through a persistent omphalomesenteric duct causing small-bowel obstruction. S Afr J Surg 50: 102-103.
13. Patel RV, Kumar H, Sinha CK, Patricolo M (2013) Neonatal prolapsed patent vitellointestinal duct. BMJ Case Rep 2013.
14. Kadian YS (2015) Patent vitellointestinal duct with inverted ileal loop prolapse: A rare presentation. Onc Gas Hep Rep 4: 95-97.
15. Fariha AF, James MN, Humdun S, Josephat N, Fred K (2017) New-born born with patent vitellointestinal duct with prolapsed (intussusceptions) of proximal and distal ileal loop: A case presentation. J Pediatr Surg Case Rep 20: 14-16.
16. Pathak A, Agarwal N, Singh P, Dhaneria M (2015) Prolapse of inverted ileal loops through a patent vitellointestinal duct. BMJ Case Rep.
Volume 13 • Issue 3 • 5J Surgery, an open access journalISSN: 1584-9341
Keywords: Intestinal malrotation; Common mesentery; Appendicitis; Laparoscopy; Appendectomy
IntroductionIntestinal malrotation is a generic term and represents any
abnormality in the rotation and fixation of the gastro-intestinal tract during its fetal development [1]. The typical 270° intestinal rotation during fetal development can occur at a wide range of locations and can lead to various acute and chronic presentations of the disease [1]. The malrotation abnormalities were reported in 1898 by Mall FP [2]. The Incidence is variable upon different studies: 1/6000 live births [3]; 0.2% in barium swallow studies in infants [3]; 1% of general population in autopsy studies [3,4]. Most of the cases were diagnosed in the first weeks of life and the presentation at adulthood is rare.
On the other hand, appendicitis is a common surgical condition, with various clinical presentations and could mimic other diseases as cholecystitis, diverticulitis, complicated ovarian cysts, and pelvic inflammatory disease. The diagnosis could be further obscured by underlying undiagnosed anatomical anomalies, for instance intestinal malrotation [5].
Case PresentationA 19 years old, young woman, BMI at 19 kg/m2, was admitted for
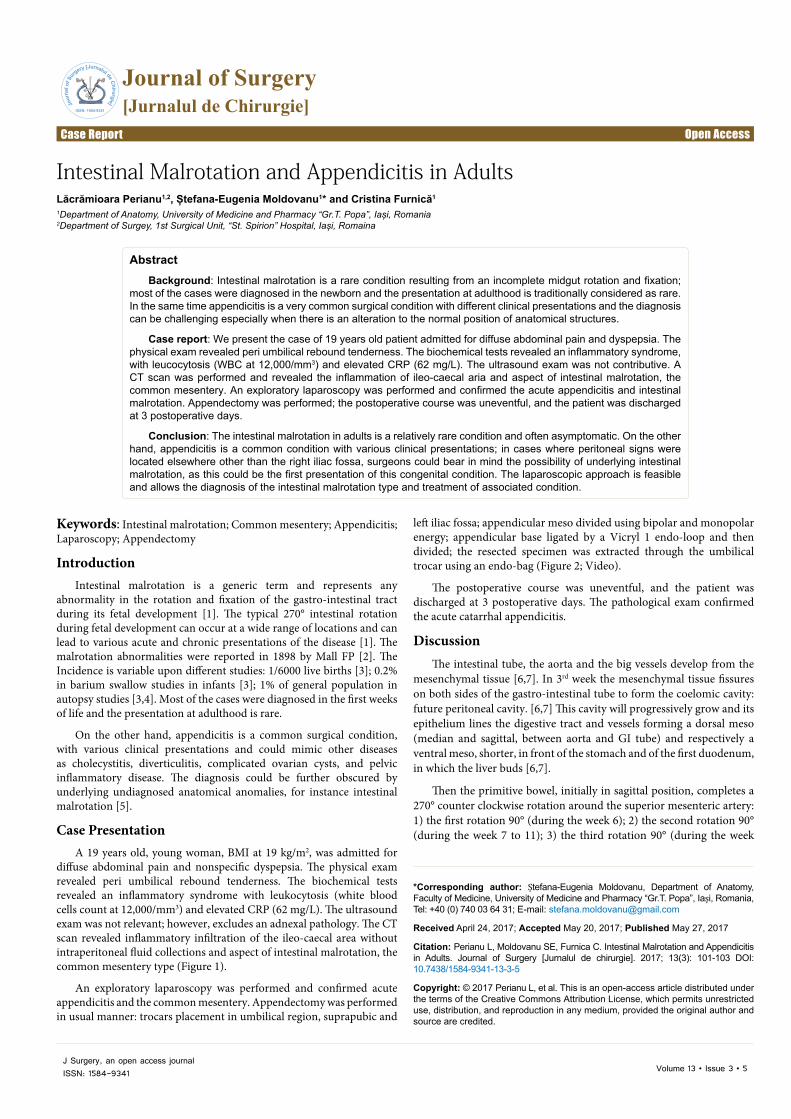
diffuse abdominal pain and nonspecific dyspepsia. The physical exam revealed peri umbilical rebound tenderness. The biochemical tests revealed an inflammatory syndrome with leukocytosis (white blood cells count at 12,000/mm3) and elevated CRP (62 mg/L). The ultrasound exam was not relevant; however, excludes an adnexal pathology. The CT scan revealed inflammatory infiltration of the ileo-caecal area without intraperitoneal fluid collections and aspect of intestinal malrotation, the common mesentery type (Figure 1).
An exploratory laparoscopy was performed and confirmed acute appendicitis and the common mesentery. Appendectomy was performed in usual manner: trocars placement in umbilical region, suprapubic and
*Corresponding author: Ștefana-Eugenia Moldovanu, Department of Anatomy, Faculty of Medicine, University of Medicine and Pharmacy “Gr.T. Popa”, Iași, Romania, Tel: +40 (0) 740 03 64 31; E-mail: [email protected]
Received April 24, 2017; Accepted May 20, 2017; Published May 27, 2017
Citation: Perianu L, Moldovanu SE, Furnica C. Intestinal Malrotation and Appendicitis in Adults. Journal of Surgery [Jurnalul de chirurgie]. 2017; 13(3): 101-103 DOI: 10.7438/1584-9341-13-3-5
AbstractBackground: Intestinal malrotation is a rare condition resulting from an incomplete midgut rotation and fixation;
most of the cases were diagnosed in the newborn and the presentation at adulthood is traditionally considered as rare. In the same time appendicitis is a very common surgical condition with different clinical presentations and the diagnosis can be challenging especially when there is an alteration to the normal position of anatomical structures.
Case report: We present the case of 19 years old patient admitted for diffuse abdominal pain and dyspepsia. The physical exam revealed peri umbilical rebound tenderness. The biochemical tests revealed an inflammatory syndrome, with leucocytosis (WBC at 12,000/mm3) and elevated CRP (62 mg/L). The ultrasound exam was not contributive. A CT scan was performed and revealed the inflammation of ileo-caecal aria and aspect of intestinal malrotation, the common mesentery. An exploratory laparoscopy was performed and confirmed the acute appendicitis and intestinal malrotation. Appendectomy was performed; the postoperative course was uneventful, and the patient was discharged at 3 postoperative days.
Conclusion: The intestinal malrotation in adults is a relatively rare condition and often asymptomatic. On the other hand, appendicitis is a common condition with various clinical presentations; in cases where peritoneal signs were located elsewhere other than the right iliac fossa, surgeons could bear in mind the possibility of underlying intestinal malrotation, as this could be the first presentation of this congenital condition. The laparoscopic approach is feasible and allows the diagnosis of the intestinal malrotation type and treatment of associated condition.
Intestinal Malrotation and Appendicitis in AdultsLăcrămioara Perianu1,2, Ștefana-Eugenia Moldovanu1* and Cristina Furnică1
1Department of Anatomy, University of Medicine and Pharmacy “Gr.T. Popa”, Iași, Romania2Department of Surgey, 1st Surgical Unit, “St. Spirion” Hospital, Iași, Romaina
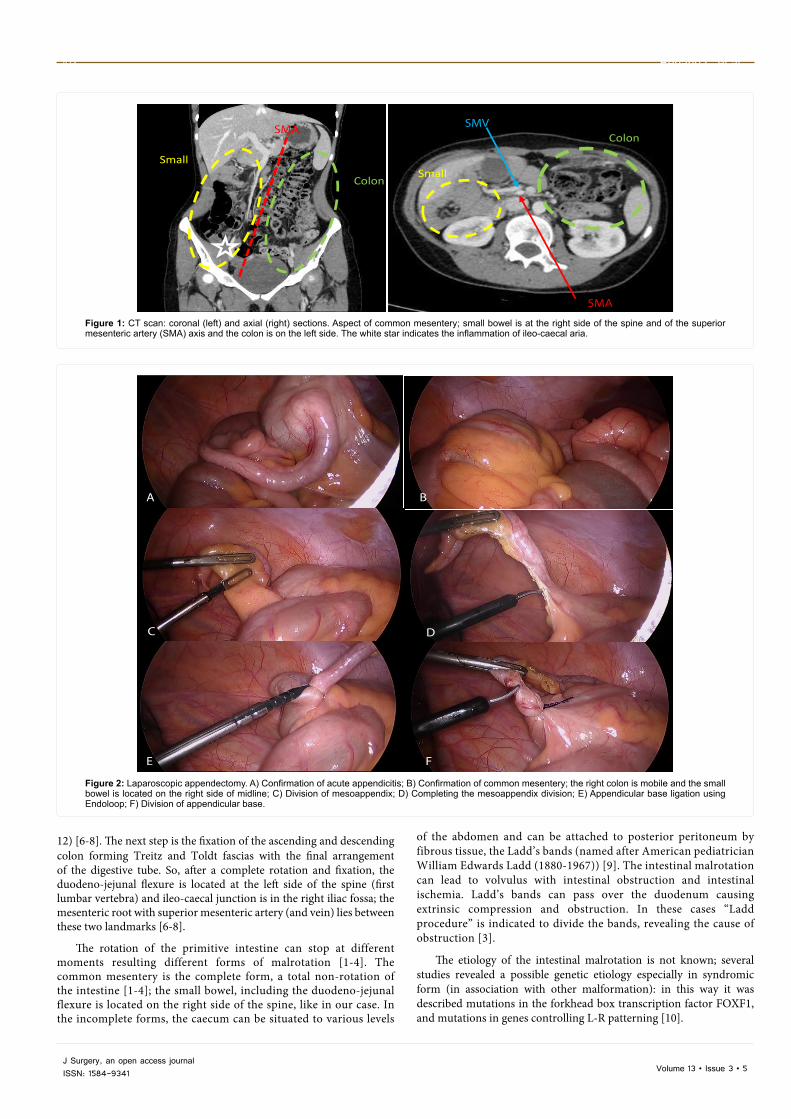
left iliac fossa; appendicular meso divided using bipolar and monopolar energy; appendicular base ligated by a Vicryl 1 endo-loop and then divided; the resected specimen was extracted through the umbilical trocar using an endo-bag (Figure 2; Video).
The postoperative course was uneventful, and the patient was discharged at 3 postoperative days. The pathological exam confirmed the acute catarrhal appendicitis.
DiscussionThe intestinal tube, the aorta and the big vessels develop from the
mesenchymal tissue [6,7]. In 3rd week the mesenchymal tissue fissures on both sides of the gastro-intestinal tube to form the coelomic cavity: future peritoneal cavity. [6,7] This cavity will progressively grow and its epithelium lines the digestive tract and vessels forming a dorsal meso (median and sagittal, between aorta and GI tube) and respectively a ventral meso, shorter, in front of the stomach and of the first duodenum, in which the liver buds [6,7].
Then the primitive bowel, initially in sagittal position, completes a 270° counter clockwise rotation around the superior mesenteric artery: 1) the first rotation 90° (during the week 6); 2) the second rotation 90° (during the week 7 to 11); 3) the third rotation 90° (during the week
Volume 13 • Issue 3 • 5J Surgery, an open access journalISSN: 1584-9341
SMA
Colon
Small bowel
SMA
SMV Colon
Small bowel
Figure 1: CT scan: coronal (left) and axial (right) sections. Aspect of common mesentery; small bowel is at the right side of the spine and of the superior mesenteric artery (SMA) axis and the colon is on the left side. The white star indicates the inflammation of ileo-caecal aria.
E F
A B
C D
Figure 2: Laparoscopic appendectomy. A) Confirmation of acute appendicitis; B) Confirmation of common mesentery; the right colon is mobile and the small bowel is located on the right side of midline; C) Division of mesoappendix; D) Completing the mesoappendix division; E) Appendicular base ligation using Endoloop; F) Division of appendicular base.
12) [6-8]. The next step is the fixation of the ascending and descending colon forming Treitz and Toldt fascias with the final arrangement of the digestive tube. So, after a complete rotation and fixation, the duodeno-jejunal flexure is located at the left side of the spine (first lumbar vertebra) and ileo-caecal junction is in the right iliac fossa; the mesenteric root with superior mesenteric artery (and vein) lies between these two landmarks [6-8].
The rotation of the primitive intestine can stop at different moments resulting different forms of malrotation [1-4]. The common mesentery is the complete form, a total non-rotation of the intestine [1-4]; the small bowel, including the duodeno-jejunal flexure is located on the right side of the spine, like in our case. In the incomplete forms, the caecum can be situated to various levels
of the abdomen and can be attached to posterior peritoneum by fibrous tissue, the Ladd’s bands (named after American pediatrician William Edwards Ladd (1880-1967)) [9]. The intestinal malrotation can lead to volvulus with intestinal obstruction and intestinal ischemia. Ladd’s bands can pass over the duodenum causing extrinsic compression and obstruction. In these cases “Ladd procedure” is indicated to divide the bands, revealing the cause of obstruction [3].
The etiology of the intestinal malrotation is not known; several studies revealed a possible genetic etiology especially in syndromic form (in association with other malformation): in this way it was described mutations in the forkhead box transcription factor FOXF1, and mutations in genes controlling L-R patterning [10].
Intestinal Malrotation 103
Volume 13 • Issue 3 • 5J Surgery, an open access journalISSN: 1584-9341
The intestinal malrotation is traditionally considered to be diagnosed in new-borns and infants [1]. However, a recent study on about 200 cases found that 31% were infants, 21% were aged 1 to 18 years, and the remaining 48% were adults [11].
Unfortunately for the new-born and infants the first sign is often the intestinal obstruction secondary to volvulus. The mortality remains elevated due to extensive intestinal ischemia [1]. In adults the diagnosis of intestinal malrotation is often an incidental finding in barium studies, angiographies, and computer tomography scans as found in literature and in our case [1,11-13].
The laparoscopic approach allows the exploration of entire abdominal cavity and diagnosis of the malrotation and of the type of malrotation, and the division of Ladd’s bands and the treatment of the associated disorder (appendectomy, as in our case, colic, or bariatric surgery) [14-17].
ConclusionThe intestinal malrotation in adults is a relatively rare condition
and often asymptomatic. On the other hand, appendicitis is a common condition with various clinical presentations; in cases where peritoneal signs were located elsewhere other than the right iliac fossa, surgeons could bear in mind the possibility of underlying intestinal malrotation, as this could be the first presentation of this congenital condition. The laparoscopic approach is feasible and allows the diagnosis of the intestinal malrotation type and treatment of associated disease.
2. Mall FP (1898) Development of the human intestine and its position in the adult. Johns Hopkins Hosp Bull 9: 197-208.
3. Holcomb GW, Murphy JD, Ostlie DJ (2014) Ashcraft's Pediatric Surgery, (6th edn.). Elsevier Health Sciences, US. pp: 430-438.
4. Kapfer SA, Rappold JF (2004) Intestinal malrotation-not just the pediatric surgeon's problem. J Am Coll Surg 199: 628-635.
5. Au A, Syed A, Bradpiece H (2010) A Rare case of intestinal malrotation presenting as appendicitis in late adulthood. J Surg Case Rep 8: 3.
6. Ifirm M, Niculescu G (1988). Compendiu de anatomie, Ed. Științifică și enciclopedică, București. pp: 32-46.
7. Tourabi AC, Raymal M, Lacombe C, Hammami W, Azizi L, et al. (2008) Imagerie des volvulus du tube digestif.
8. Nabavizadeh A (2014) Embriological Rotation of the Midgut. University of Chicago Pritzker School of Medicine.
9. Browne NT, Flanigan LM, McComiskey CA, Nancy PP (2007) Nursing care of the pediatric surgical patient (3rd edn.). Jones & Bartlett Learning, US. pp: 334.
10. Martin V, Shaw-Smith C (2010) Review of genetic factors in intestinal malrotation. Pediatr Surg Int 26: 769-781.
11. Nehra D, Goldstein AM (2011) Intestinal malrotation: Varied clinical presentation from infancy through adulthood. Surgery 149: 386-93.
12. Shahverdi E, Morshedi M, Allahverdi KM, Baradaran JM, Shafizadeh BF (2017) Utility of the CT scan in Diagnosing Midgut Volvulus in Patients with Chronic Abdominal Pain. Case Rep Surg 2017: 1079192.
13. Husberg B, Salehi K, Peters T, Gunnarsson U, Michanek M, et al. (2016) Congenital intestinal malrotation in adolescent and adult patients: A 12-year clinical and radiological survey. Springerplus 5: 245.
14. Coulibaly M, Boukatta B, Derkaoui A, Sbai H, Ousadden A, et al. (2015) Volvulus du grêle sur mésentère commun incomplet-une redoutable complication rare chez l’adulte: à propos de 1 cas. Pan African Medical Journal 20: 157.
15. Flesch J, Oswald P, Grebici M, Schmaltz C, Bruant P, et al. (2010) Common mesentery presenting with left-sided perforated appendicitis. J Radiol 91: 915-6.
16. Nishida K, Kato T, Lefor AK, Suganuma T (2017) Laparoscopic resection of sigmoid colon cancer with intestinal malrotation: A case report. Int J Surg Case Rep 34: 77-80.
17. Vidal EA, Rendon FA, Zambrano TA, García YA, Viteri MF, et al. (2016) Intestinal malrotation in patients undergoing bariatric surgery. Arq Bras Cir Dig 29: 24-26.
IntroductionParotid gland tumors account for 80% of all salivary gland neoplasms,
20% of these are malignant, but in daily clinical practice most parotid masses are operated on before obtaining the final histological diagnosis [1]. This clinical setting further complicates the critical point of parotid surgery, which is the management of the facial nerve [2]. We present herein a case of parotid tumor treated by parotidectomy.
Case PresentationThe patient, 54 years old male presented with the following signs
and symptoms: left tumoral mass, solid and pain and discomfort, despite he had underwent parotidectomy 1 year ago. The tumor was located in front part of the left ear and had 3.5 cm. MRI and CT scan confirmed recurrence of the tumor.
The patient's head was turned away from the side of the tumor and the neck extended (arched back). The incision started in front of the left ear, curved around the bottom of the ear and then down the posterior aspect of the jawbone (Figure 1). An anterior subplatysmal/subsuperficial musculoaponeurotic system (SMAS) flap is made by using the natural plane on the surface of the parotid gland. The ear lobe was lifted-up and backward and the posterior border of the parotid gland was exposed first (Figure 1).
The case was difficult and required attention, because the trajectory of the facial nerve was through the left parotid gland. This could explain the recurrence of tumor due to surrounding tissues with the tumor. Finally, we identified the facial nerve trunk and its branches. We removed the superficial lobe first, and then dissected out of the deep lobe between the branches of the facial nerve. We paid attention not to injure the facial nerve branches. As we can see in Figure 2, the facial nerve is white and looks like a plant root. We removed carefully the tumor, process that took us 2 hours (Figures 2 and 3). After that, the drainage tube was placed to prevent hematoma. The patient was discharged the third day with no fistula or any other complication (Figure 4).
DiscussionSalivary cancers account for approximately 3% of all head and
neck malignancies diagnosed in the United States each year; most of these (80%) are located in the parotid glands. Most benign tumors of the parotid gland are epithelial tumors. Pleomorphic adenoma is the most common tumor of the parotid gland (60 to 70% of all tumors) [1,2]. The pleomorphic adenoma is a benign tumor with a potential for local recurrence [2-4] and an extremely low rate of malignant transformation (1-2% of primary parotid gland malignancy) [5,6].
*Corresponding author: Abbas El Husseini, Dar Al Amal Hospital, Baalbeck, Beirut, Douris (Baalbeck), Lebanon, Tel: +961 8 371 901; E-mail: [email protected]
Received July 04, 2017; Accepted July 25, 2017; Published August 01, 2017
Citation: El Husseini M, El Husseini A. Parotidectomy in a 54 Years Old Patient: Case Report. Journal of Surgery [Jurnalul de chirurgie]. 2017; 13(3): 105-107 DOI: 10.7438/1584-9341-13-3-6
AbstractParotid gland tumors account for 80% of all salivary gland neoplasms, 20% of these are malignant, but in daily
clinical practice most parotid masses are operated on before obtaining the final histological diagnosis. This clinical setting further complicates the critical point of parotid surgery, which is the management of the facial nerve. We present the case of 54 years old male patient diagnosed with parotid tumor. He underwent a parotidectomy and the postoperative course was uneventful. Different key points of management and of the surgical procedure are highlighted and discussed.
Parotidectomy in a 54 Years Old Patient: Case ReportMohamed El Husseini and Abbas El Husseini*Dar Al Amal Hospital, Baalbeck, Beirut, Lebanon
Surgery is the main treatment of pleomorphic adenoma. Enucleation is no longer recommended [1,4-6]. In patients with pleomorphic adenoma of the superficial lobe, either superficial or total parotidectomy can be used. Superficial parotidectomy may be associated with a higher recurrence rate and total parotidectomy with a higher risk of facial nerve dysfunction [7,8].
The parotid gland is shaped like an upside-down triangle and lies in front and below the opening to the ear canal [9]. Anterior is the posterior surface of the jawbone and the masseter muscle. The deep surface of the gland lies alongside the back of the throat, near the tonsils. The gland is divided by the facial nerve into a superficial and deep lobe. The facial nerve arises in the skull, emerges at the stylomastoid foramen, enters the gland and branches out inside the parotid, defining the superficial
Figure 1: Parotidectomy: dissecting the skin and underlying layers.
Volume 13 • Issue 3 • 6J Surgery, an open access journalISSN: 1584-9341
and the deep lobe, and must always be identified and dissected when performing parotidectomy. It supplies the muscles of the face. Surgical landmarks to the facial nerve include the tympanomastoid suture line, the tragal pointer, and the posterior belly of the digastric muscle. The tympanomastoid suture line lies between the mastoid and tympanic segments of the temporal bone and is approximately 6-8 mm lateral to the stylomastoid foramen. The main trunk of the nerve can also be found midway between (10 mm posteroinferior to) the cartilaginous tragal pointer of the external auditory canal and the posterior belly of the digastric muscle.
Pathology of parotid glands includes inflammation and infection conditions (stones, abscess) and tumors of the parotid. 70-80% of parotid tumors are benign, the most common being the pleomorphic adenoma and Warthin's tumor. Cancer of the parotid gland occurs in about 20-25% of parotid tumors.
The physical examination is the first diagnostic tool. Most benign parotid tumors present as slow growing, painless masses often in the tail of the parotid gland. Ultrasonography has a high sensitivity in detecting masses in the superficial lobe of the parotid gland. Computerized tomography and/or magnetic resonance imaging reveal the deeper parotid lobe. Fine-needle aspiration biopsy (FNAB) is also indicated by some authors [10-12]. Open biopsy of a parotid mass is not recommended due to the risk of seeding in the case of solid malignancy. Therefore, what usually occurs in clinical practice is that most parotid masses are operated upon in order to obtain the final histological diagnosis.
Surgery of the parotid gland is challenging because the VII cranial nerve. Dissection of the branches of the facial nerve requires patience and special attention both to detail and to landmarks [13]. When the course of a nerve is distorted and attenuated by a tumor, preservation of facial nerve fibers can be very difficult. Experience shows that most of the primary salivary tumors of the parotid are found directly adjacent to at least one branch of the facial nerve.
So, in our opinion, the most conservative operation should be superficial parotidectomy, also in the case of a clearly benign mass. Furthermore, in the event of recurrence, the risk to the facial nerve increases exponentially, particularly in the relatively frequent event of a multi-nodular relapse of a pleomorphic adenoma [14].
Enucleation should be done only in Warthin tumors especially when presenting posterior to the facial nerve [15].
Potential complications of parotidectomy include facial nerve injury, Frey syndrome (the patient may experience sweating or flushing of the skin over the parotid gland every time he eats), salivary leakage, ear numbness, facial asymmetry, flap necrosis, and tumor recurrence.
There may be some weakness of the facial muscles on the side of the surgery due to swelling of the tissues around the nerve. This usually resolves in a few days. Radiation therapy may sometimes be necessary if the tumor was very large, involved nearby tissues or lymph nodes or in cases of deep lobe tumors; as it is sometimes difficult to assess the full extent of the dissection. The prognosis varies with the pathologic type, the size of the tumor and the spread of tumor to surrounding tissues.
ConclusionPreoperative investigation includes a minimum of FNA and MRI
(contrast enhanced CT is a reasonable alternative in cases where MRI is contraindicated), which inform patient counseling and discussion of adjuvant radiotherapy. The extent of surgery is dictated by the site and size of the tumor and involves a form of superficial or total conservative parotidectomy with preservation of a functioning facial nerve.
Conflict of Interest
Authors have no conflict of interest to disclose.
References
1. Laccourreye H, Laccourreye O, Cauchois R, Jouffre V, Menard M, et al. (1994) Total conservative parotidectomy for primary benign pleomorphic adenoma of the parotid gland: A 25-year experience with 229 patients. Laryngoscope 104: 1487-1494.
2. Mc Gurk M, Renehan A, Gleave EN, Hancock BD (1996) Clinical significance of the tumour capsule in the treatment of parotid pleomorphic adenomas. Br J Surg 83: 1747-1749.
3. Froehlich P, Fombeur JP, Vuong PN (1991) Treatment of recurrence of pleomorphic adenomas of the parotid gland. Ann Otolaryngol Chir Cervicofac 108: 333-337.
Figure 2: Exposure of the facial nerve.
Figure 3: The resected specimen.
Figure 4: Final aspect; to note the vacuum drain to avoid hematoma.
Volume 13 • Issue 3 • 6J Surgery, an open access journalISSN: 1584-9341
4. Laskawi R, Schott T, Schroder M (1998) Recurrent pleomorphic adenomas of the parotid gland: clinical evaluation and long-term follow-up. Br J Oral Maxillofac Surg 36: 48-51.
5. Chevalier D, Loche V, Darras JA, Apko-Allavo J, Desaulty A, et al. (1996) Reoperation and recurrence of pleomorphic adenoma of the parotid. A propos of 62 cases. Ann Otolaryngol Chir Cervicofac 113: 56-60.
6. Myssiorek D, Ruah CB, Hybels RL (1990) Recurrent pleomorphic adenomas of the parotid gland. Head Neck 12: 332-336.
7. Becelli R, Perugini M, Mastellone P, Frati R (2001) Surgical treatment of recurrences of pleomorphic adenoma of the parotid gland. J Exp Clin Cancer Res 20: 487-489.
8. Carew JF, Spiro RH, Singh B, Shah JP (1999) Treatment of recurrent pleomorphic adenomas of the parotid gland. Otolaryngol Head Neck Surg 121: 539-542.
10. Zbaren P, Schar C, Hotz MA, Loosli H (2001) Value of fine-needle aspiration cytology of parotid gland masses. Laryngoscope 111: 1989-1992.
11. Sergi B, Contucci AM, Corina L Paludetti G (2004) Value of fine-needle aspiration cytology of parotid gland masses. Laryngoscope 114: 789-789.
12. Contucci AM, Corina L, Sergi B, Fadda G, Paludetti G (2003) Correlation between fine needle aspiration biopsy and histologic findings in parotid masses. Personal experience. Acta Otorhinolaryngol Ital 23: 314-318.
13. Rea PM, McGarry G, Shaw-Dunn J (2010) The precision of four commonly used surgical landmarks for locating the facial nerve in anterograde parotidectomy in humans. Ann Anat 192: 27-32.
14. Redaelli de Zinis LO, Piccioni M, Antonelli AR, Piero N (2008) Management and prognostic factors of recurrent pleomorphic adenoma of the parotid gland: personal experience and review of the literature. Eur Arch Otorhinolaryngol 265: 447-452.
15. Heller KS, Attie JN (1988) Treatment of Warthin's tumor by enucleation. Am J Surg 156: 294-296.